Download
1 / 57
610 likes | 1.1k Views
ABNORMALITIES OF SMELL. PRESENTED BY: SHARWARI BAKRE. Patients may simply complain that they have lost the ability to smell. Alternatively complex descriptions may be presented which can obscure the real pattern of the abnormality.

E N D
Patients may simply complain that they have lost the ability to smell. Alternatively complex descriptions may be presented which can obscure the real pattern of the abnormality.
It is important for a classification to be questioned accordingly to avoid the vagueness which often impedes a proper understanding when perceptive problems are considered.
In the Ayurvedic classics references regarding gandha dnyana hani are as follows. The following diseases having gandha dnyana hani. 1.RaktajaPratishyaya 2.DushtaPratishyaya 3. Pinasa
Hetu for NasaRog:1.Vegavidharan(chardi etc.)2.Ajirna3.Dhuma4.Atibhashya5.Krodha6.Rutuviparyay7.Shirobhitap8. Ratrijagarana
.9.Diwaswapa10.Ambu11.Avashayay 12.Maithuna13.Bashapa14.Dhumsevan15.Piten anyenvarina
Raktaja PratishyayaDurgandho chwasadan astatha gandhanna vetticha.Ref. Su.U.24/12-13
Dusthata PratishyayaNishswasochwasdaurgandhyam tatha gandhanna vettichaRef. Su.U.24/14-15Cha.chi.26
PinasaNa vetti yogandharasanschajanturjushtamvyavasyettampinasenaRef. Su.U.22/6
Sadharana Chikitsa1.Ghuta pan 2.Swedan3.Vamana (vata-kaphaja)4.Avapida
Pakva Pratishaya1.ShiroVirechan2.Virechan 3.Aasthapan4.Dhumrapan 5.Kavala ghraha6.Nivatasthana7.ShiroVirechanNasya8.Tikshana Nasya9.Ruksha Yavanna10.Haritaki Sevan
Vishesha Chikitsa1) Raktaja Pratishyayaa) KakollyadisiddhaGhutab) SheetalParishekac)Pand)Pradehae)Kavalaf) Virechan
2)Dusthata Pratishyayaa)Yakshamanashaka, Kruminashaka Chikitsaeg: Gomutra, Surasaetc.
3)Pinasaa) Following draya are used in preparation of Varti : Trikatu, Vidanga, Devdaru, Kusta, Trivrut, Shigruphala, etc.Dhumapan of such Varti is done
According to Modern ScienceThe following arrangment may be found to be useful.1. Quantitative Changea) Decreased sensitivity to smell1)Anosmia : The loss of sense of smell2) Hyposmia : Reduced sense of smellb)Increased sensitivity to smell1.Hyperosmia
2.Qualitative Changesa) Peripheral Type 1.Local causes2.Anosmic zones3. Singlenon-discriminating response 4.Essential parosmia5.Cacosmiab) Central Type1.Illusion 2. Hallucination 3.Abnormal sense memory.
1.Anosmia : Inability to detect qualitative olfactory sensations absence of smell function. 2.Hyposmia : Decreased sensitivity to odorants .3.Hyperosmia : Abnormally acute smell function .4. Dysosmia : Distorted or perverted smell perception.5.Olfactory Agnosia : Inability to recognize an odor sensetion.
The etiology of most cases of olfactory dysfunction can be ascertained from carefully questioning the patient about the nature, timing, onset, duration and pattern of their symptoms.
1.Historical determination of antecedent events.2.History of sinonasal disease and allergic symptoms.3.Smoking history.4.Occupational history.5.The physical examination should focus on the neurologic system and intranasal anatomy.
6.Nasal endoscopy – examined for nasal masses, polyps, exudates etc7.Radiographic studies for specific indications.
8. C.T. Scan is ideal for investigation of nasal and sinus disease.9. MRI is for intracranial pathology.10. Olfactory test : Smell identification test.
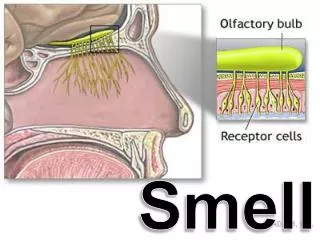
YesLike all our senses, our sense of smell plays an important part in our lives.Sense of smell often serves as a first warning signal, alerting us to the smoke of fire.The odor of a natural gas leak and dangerous fumes.
Yes- Some people experience relief from smell disorders.- Since certain medication can cause a problem, adjusting or changing that medicine may ease its effects on the sense of smell. - Others recover their ability to smell when the illness causing their olfactory problem resolves.
- For patients with nasal obstructions such as polyps, surgery can remove the obstructions and restore airflow.- People enjoy a spontaneous recovery because olfactory neurons may regenerate following damage.
Anosmia and HyposmiaWhen there is a loss of the sense of smell, the flavour is also not perceived. The food may have an insipid taste, as only the 4 basic tastes remain.
2. Respiratory anosmia : severe anatomical deformities in the nose which prevent the inhaled air containing odoriferous particles from entering the olfactory area may cause full loss of sense of smell. This condition is called respiratory anosmia.
3. Essential anosmia : Total loss of smell due to olfactory nerve affection.4. Central anosmia : Anosmia sometimes produced by pathological condition in the brain such as cerebral abscess, tumor or encephalitis known as central anosmia.
1. Nose a) Obtructions which prevent the odour reaching to the olfactory area like deviated nasal septum, polyps , hypertrophic turbinates and neoplasms b) Rhinitis c) Allergic and vasomotor rhinitis d)Atrophic rhinitis e) Bromine fumes
2.Neurologicala.Traumatic : fractures of the base of the skull involving the olfactory area of the brain and olfactory nerves.b. Peripheral neuritis as in diabetis, syphilis and influenza.c. Intracranial lesions like abscess tumours and meningitis affecting olfactory tracts and centers.d. Senile atrophy may be a cause.
In respiratory anosmia, the prognosis is favorable, since the olfactory sense may be restored by removing the mechanical obstacle to respiration. In essential anosmia, the forecast is usually hopeless, as the dead nerve ending cannot be vitalized. In central anosmia, the prognosis depends on the nature of the basic disorder and is often unfavorable.
Treatment should be directed towards the removal of obstacles leading to the olfactory fissure. In essential and central anosmia the basic requirement is to cure the principal disease.
Intrinsic causes as follows :1.Maxillary sinusities of dental origin.2.Foreign bodies in the nose.3.Foul smelling pus in the middle ear cleft.4.Lung abscess.5. Dental infection.6. Malignancy.
Causes : 1. Functional 2. Neurological – Peripheral neuritis, epileptic, aura, uncinate fits.3.Drugs like streptomycin etc.
In the cases of conductive loss, treatment is directed at relieving the physical obstruction arise from several causes including allergic rhinitis, polyps, chronic sinusitis.
Effective treatment for olfactory loss secondary to allergic rhinitis include allergy management, topical cromolyn and surgical procedures to reduce inflammation or obstruction.
Surgery is indicated to treat the obstructed breathing and to improve smell function.
In patient who remain anosmic after surgery for nasal and sinus polyps, studies have shown that oral steroids were effective in restoring smell function to normal in most patients.
Olfactory dysfunction secondary to sensorineural causes is difficult to manage. Prognosis is generally poor.