Download
1 / 8
80 likes | 186 Views
Poster Discussion GI Non-CRC ASCO 2008 Abstracts 4524-4530. John L. Marshall, MD Chief, Division Hematology and Oncology Lombardi Comprehensive Cancer Center Georgetown University Washington DC. Where we are with UGI Cancers…. Accepting a 10-20% response rate as good, arguably exciting

E N D
Poster DiscussionGI Non-CRCASCO 2008Abstracts 4524-4530 John L. Marshall, MD Chief, Division Hematology and Oncology Lombardi Comprehensive Cancer Center Georgetown University Washington DC
Where we are with UGI Cancers…. • Accepting a 10-20% response rate as good, arguably exciting • Treat everyone the same in the hope they are in the 10-20%
Where we are with Breast and Colon Cancers…. • Breast Cancer- now multiple diseases • ER/PR • HER2 • Triple Negative • BRCA +/- • Colon- now at least 2 diseases • KRAS WT • KRAS Mutant • MSI, 18q?
Pathways to Discovery New Drug Large Trial Positive Results Retrospective Tumor Analysis
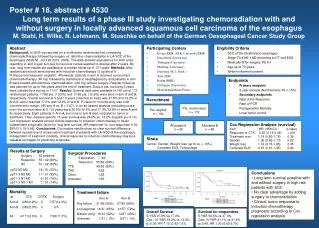
Abstract Themes • Cancer Origins • Barrett’s (Cen et al) • Hereditary diffuse gastric cancer (Shah et al) • Molecular Targets • HER2 (Bang et al) • Tumor/Host Interactions • Regulatory T cells (Graziano et al) • Optimizing Staging • Number of lymph nodes (Groth et al) • PET Scan as a predictor (Vallbohmer et al) • Role of surgery (Stahl et al)
Nuklearmedizin. 2007;46(6):263-70. Links • Visualisation of metastatic oesophageal and gastric cancer and prediction of clinical response to palliative chemotherapy using 18FDG PET. • Lorenzen S, Herrmann K, Weber WA, Wieder H, Hennig M, Ott K, Bredenkamp R, Peschel C, Schwaiger M, Lordick F. • 3rd Department of Internal Medicine (Haematology/Medical Oncology), Klinikum rechts der Isar, Technical University, Ismaninger Strasse 22, Munich, Germany. • AIM: This study assessed the value of (18)F-deoxyglucose positron emission tomography (FDG-PET) for visualisation and early metabolic response assessment in metastatic gastro-oesophageal cancer. PATIENTS, METHODS: Twenty-six patients who were treated for metastatic disease (20 adenocarcinomas, 6 squamous cell cancers) underwent FDG-PET before and two weeks after the onset of palliative chemotherapy with either oxaliplatin + 5-FU/LV or with docetaxel + capecitabine. PET results were validated according to clinical response based on RECIST criteria. RESULTS: Twenty-four tumours (92%) could be visualised by FDG-PET and were also assessable by a second PET scan at 2 weeks. The 2 tumours that were not detectable by PET were both gastric cancers belonging to the non-intestinal subtype according to Lauren. Median time to progression and overall survival were not significantly different for metabolic responders and non-responders (6.3 vs 5.3 months and 14.1 vs 12.5 months, respectively). CONCLUSION: In this heterogeneous study population, FDG-PET had a limited accuracy in predicting clinical response. However, the metabolic response prediction was particularly good in the subgroup of patients with oesophageal squamous cell cancer. Therefore, FDG-PET and assessment of cancer therapy clearly merits further investigation in circumscribed patient populations with metastatic disease.
Lancet Oncol. 2007 Sep;8(9):797-805. Links • Comment in: • Lancet Oncol. 2007 Sep;8(9):754-5. • PET to assess early metabolic response and to guide treatment of adenocarcinoma of the oesophagogastric junction: the MUNICON phase II trial. • Lordick F, Ott K, Krause BJ, Weber WA, Becker K, Stein HJ, Lorenzen S, Schuster T, Wieder H, Herrmann K, Bredenkamp R, Höfler H, Fink U, Peschel C, Schwaiger M, Siewert JR. • Department of Surgery, Clinic rechts der Isar, Technical University of Munich, Munich, Germany. florian.lordick@med.uni-heidelberg.de • BACKGROUND: In patients with locally advanced adenocarcinoma of the oesophagogastric junction (AEG), early metabolic response defined by 18-fluorodeoxyglucose-PET ([(18)F]FDG-PET) during neoadjuvant chemotherapy is predictive of histopathological response and survival. We aimed to assess the feasibility of a PET-response-guided treatment algorithm and its potential effect on prognosis. METHODS: Between May 27, 2002, and Aug 4, 2005, 119 patients with locally advanced adenocarcinoma of AEG type 1 (distal oesophageal adenocarcinoma) or type 2 (gastric cardia adenocarcinoma) were recruited into this prospective, single-centre study. All patients were assigned to 2 weeks of platinum and fluorouracil-based induction chemotherapy (evaluation period). Those with decreases in tumour glucose standard uptake values (SUVs), predefined as decreases of 35% or more at the end of the evaluation period and measured by PET, were defined as metabolic responders. Responders continued to receive neoadjuvant chemotherapy of folinic acid and fluorouracil plus cisplatin, or folinic acid and fluorouracil plus cisplatin and paclitaxel, or folinic acid and fluorouracil plus oxaliplatin for 12 weeks and then proceeded to surgery. Metabolic non-responders discontinued chemotherapy after the 2-week evaluation period and proceeded to surgery. The primary endpoint was median overall survival of metabolic responders and non-responders. Secondary endpoints were median event-free survival, postoperative complications and mortality, number of residual tumour-free (R0) resections, and histopathological responses. This study has been registered in the European Clinical Trials Database (EudraCT) as trial 2007-003356-11. FINDINGS: 110 patients were evaluable for metabolic responses. 54 of these patients had metabolic responses (ie, decrease of 35% or more in tumour glucose SUV) after 2 weeks of induction chemotherapy, corresponding to a response of 49% (95% CI 39-59). 104 patients had tumour resection (50 in the responder group and 54 in the non-responder group). After a median follow-up of 2.3 years (IQR 1.7-3.0), median overall survival was not reached in metabolic responders, whereas median overall survival was 25.8 months (19.4-32.2) in non-responders (HR 2.13 [1.14-3.99, p=0.015). Median event-free survival was 29.7 months (95% CI 23.6-35.7) in metabolic responders and 14.1 months (7.5-20.6) in non-responders (hazard ratio [HR] 2.18 [1.32-3.62], p=0.002). Major histological remissions (<10% residual tumour) were noted in 29 of 50 metabolic responders (58% [95% CI 48-67]), but no histological response was noted in metabolic non-responders. INTERPRETATION: This study confirmed prospectively the usefulness of early metabolic response evaluation, and shows the feasibility of a PET-guided treatment algorithm. These findings might enable tailoring of multimodal treatment in accordance with individual tumour biology in future randomised trials.
Eur J Nucl Med Mol Imaging. 2007 Dec;34(12):1925-32. Epub 2007 Aug 7. Links • Prediction of tumor response by FDG-PET: comparison of the accuracy of single and sequential studies in patients with adenocarcinomas of the esophagogastric junction. • Wieder HA, Ott K, Lordick F, Becker K, Stahl A, Herrmann K, Fink U, Siewert JR, Schwaiger M, Weber WA. • Department of Nuclear Medicine, Klinikum rechts der Isar, Technische Universitaet Muenchen, Ismaningerstrasse 22, Munich, Germany. h@wieder.de • PURPOSE: Positron-emission-tomography with the glucose analog fluorodeoxyglucose (FDG-PET) has shown encouraging results for prediction of tumor response to chemotherapy. However, there is no consensus as to what time after initiation of therapy FDG-PET should be performed. To address this question we studied the time course of changes in tumor FDG-uptake in patients with locally advanced adenocarcinomas of the esophagogastric junction (AEG) treated with preoperative chemotherapy. METHODS: Twenty-four patients with AEG were included and underwent FDG-PET prior to therapy (PET1), 2 weeks after initiation of therapy (PET2), and preoperatively (PET3). Tumor metabolic activity was assessed by standardized uptake values (SUV) and correlated with histopathologic response and patient survival. RESULTS: Baseline tumor SUV was 8.3 +/- 3.5 and decreased to 5.0 +/- 1.8 at PET2 (p < 0.0001). At PET3 there was further decrease to 3.5 +/- 1.9 (p < 0.0001). The relative decrease of tumor FDG-uptake from PET1 to PET2 and from PET1 to PET3 were both significantly correlated with histopathologic response. Reduction of tumor SUV from PET1 to PET2 was significantly correlated with survival (p = 0.03) and there was a similar trend for changes from PET1 to PET3 (p = 0.09). In contrast, absolute SUVs did not demonstrate a significant correlation with histopathological response or patient survival at any of the studied time points. CONCLUSION: In patients with AEG, relative changes in tumor FDG uptake are better predictors for treatment outcome than absolute SUVs. Metabolic changes within the first 2 weeks of therapy are at least as efficient for prediction of histopathologic response and patient survival as later changes.