Download
1 / 28
630 likes | 2.94k Views
Fall from Height. Falls from height. 30-40% associated with suicidal intent Remainder accidental Seasonal variation in accidental falls Suicidal attempts show no such seasonal variation Also associated with drugs, alcohol and psychiatric disease.

E N D
Falls from height • 30-40% associated with suicidal intent • Remainder accidental • Seasonal variation in accidental falls • Suicidal attempts show no such seasonal variation • Also associated with drugs, alcohol and psychiatric disease
Can the Distance Fallen Predict Serious Injury after a Fall from a Height? • J Trauma, Volume 46(6). June 1999.1055-1058 • Impact (v) is related to the Height fallen (h) and acceleration due to Gravity (g, 9.8m·sec-2) • ATLS Fall >20 feet(6.1M): a clinically important risk, above which major trauma is considered • total of 166 cases; 141 males and 25 females.Height of fall: 1 to 20 meters; Mean height fallen was 3.2 meters
Can the Distance Fallen Predict Serious Injury after a Fall from a Height? • As a sole criterion, height of fall is a poor predictor of major injury • Sensitivity is inadequate to rule out major injury • Positive predictive value of the test is poor • The relative risk of serious injury increases with age • Those who landed on heads had an increased relative risk • Conclusions • Any trauma victim who has fallen more than 2 meters (6.6 feet) is at significant risk of serious injury. • The height of fall should not be used as a sole criterion for trauma triage decision-making.
Prognostic factors in victims of falls from height Crit Care Med 2005; 33:1239-1242 Patient age, height of fall, circumstances of fall, and the body part first touching the ground are independent prognostic factors in victims of falls from height Out-ofhospital mortality comprised 70% of the total mortality, including 56% of the patients who died immediately on site A strong correlation between height of fall and mortality. The median height of fall in patients who died: 15 m, 5 floors
Prognostic factors in victims of falls from height The nature of the impact surface Survival after fall from 96 m, with a 28 m·sec-1 velocity at contact, and deceleration estimated at 191 G on a beach WWII, pilot jumped from plane at 7320 m and landed in pine forest and snow: the survivor of the most extraordinary free fall ever reported Falls from height into water: Impact of feet on the water, deceleration force is around 6 G. In cases of lateral impact, this force reaches 40 G
Prognostic factors in victims of falls from height On a solid impact surface, body orientation at the time of the impact was a theoretical prognostic factor Impact on the feet results in lower extremity trauma which is not life threatening in most cases. In contrast, injuries after impact on the head are clearly life threatening. Mortality rate: 57% in ventral impact; 23% after dorsal impact Because of the head weight, children are particularly predisposed to cranial trauma.
Postmortem Analysis of Fatal Falls • The head is the most frequently injured body region (70%), followed by the chest, abdomen, extremities, and neck • Primary cause of death was craniocerebral trauma and that the vast majority of skull injuries associated with falls down stairs were found above the “hat brim line.” • Aortic lacerations and vertebral compression fractures were also frequent.
The Physics of Falling • Falls are examples of vertical deceleration injuries (VDI) • Patterns of injury differ from horizontal deceleration injuries (HDI) associated with motor vehicle accidents • Fractures and retro-peritoneal injuries are more common in VDIs • Intra-abdominal injuries are more common in HDIs
The Physics of Falling • Factors influencing magnitude of injury: • Impact velocity • Rate of deceleration • Impact surface • Body habitus • Age of patient • Orientation of body on impact • Objects encountered during fall (associated with upper limb fractures)
Patterns of Injury in Victims of Urban Free-Falls • Major damage to parenchymal organs of the abdominal and thoracic cavity is the predominant cause of death after falls from extreme heights. • Scalea et al. • J. Trauma 26:706, 1981 • Mechanisms sufficient to cause serious damage to intra-abdominal organs are severe enough to cause other injuries resulting in immediate death. • Retroperitoneum is the most likely source of hemodynamic instability, and they therefore recommended transportation to the angiography suite rather than the operating room for fall victims with evidence of continuous blood loss.
Patterns of Injury in Victims of Urban Free-Falls • ARDS may occur owing to direct transmission of shear forces to the alveoli after acute vertical deceleration. • Peripheral vascular injuries are rare but should not be overlooked. • Usually consist of intimal tears or pseudoaneurysms • Always associated with falls of more than 30 feet and fractures of the corresponding extremity. • The popliteal artery is most commonly involved.
Patterns of Injury in Victims of Urban Free-Falls • Survival is rare after urban free-falls from heights > 40 feet • Spinal injuries may occur after falls from any height and a low threshold for aggressive evaluation of the whole spine should be adopted, especially in the presence of associated lower extremity fractures. • Intraabdominal organ injuries are not uncommon and should be prioritized before retroperitoneal trauma in the differential diagnosis of the hemodynamically unstable fall victim. • Major vascular injuries are rare in survivors from urban falls but should be suspected and treated promptly for optimal results. • The height of the fall is a good predictor of injury severity and ultimate outcome.
Patterns of Injury in Victims of Urban Free-Falls • The “battleship fracture”—simultaneous fracture of the lumbar spine and a tarsal or metatarsal bone. • Two-thirds of patients with a fracture in the foot also had a lumbar spine fracture. • All patients with spine fractures in whom the GCS was 14 or 15 had positive physical findings of their spinal fracture: pain, palpation tenderness, or neurologic deficits. • Bypass extensive spinal radiographs in patients who clearly are awake and alert and have a negative physical examination.
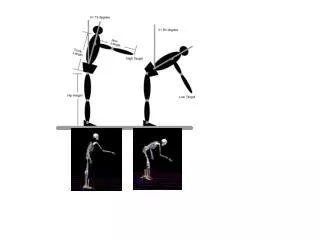
Head-First Falls: • Hyperextension of the head. • Compression of the cervical spine. • Chest, lower spine and pelvic injuries are also common.
Feet-First Falls • Compression travels up the spinal column. • Falls greater than 20ft. possible affect on internal organs. • Foreword falls look for Colles’ or silver fork fractures of the wrist. • Thrown backwards look for injuries to head, back, and pelvis.
Calcaneal fractures • Diagnosis • Bohler’s salient angle < 20 degrees suggests fracture • 7 common fracture patterns • Treatment • Need CT to assess involvement of sub-talar joint • Can be surgically reconstructed or managed conservatively
Pelvic Fractures • Common in buttock and feet first landings • Occur in 20-30% of all falls from height • As with other fractures, has been shown to increased in frequency with increasing height of fall • All types of pelvic fractures described
Thoraco-lumbar fractures • Commonest skeletal fracture associated with falls with an incidence of 80% • Thoracolumbar junction is area most often involved • L1 > L2 > T12 • Stability depends upon column theory • CT useful in determining stability
Cervical Spine Fractures • Rare in falls • Can be seen with feet first landings with flexion of the neck at impact • Flexion type cervical spine fractures: • Anterior subluxation • Bilateral facet joint dislocation • Wedge / compression fracture • Clay-shoveler fracture
Pediatric Falls from Height How common are falls ? • Roughly half < 1yr fall from height • Frequent source of ED Visits (≈1/100/yr) • Frequent source of hospitalization (≈ 1/1000/yr) • Infrequent cause of death (≈ 4/1,000,000/yr)
Body Orientation on Impact • Determines the pattern of injuries sustained • Determines mortality rate • Head first • 50% mortality from 1 floor • Feet first • 50% mortality from 5 floors • Horizontal landing • Associated with chest and abdominal injuries
Feet First Landing • Commonest orientation on landing • Associated with typical fracture distribution: • Calcaneus and subtalar joint • Tibial plateau and fibula • Femur • Pelvis • Lumbar spine • Thoracic and cervical spine
Free Falls & Fatality • Deaths from falls in children: how far is fatal? J Trauma. 1991; 31:1353-1355. • Fatalities: 10-45ft 1/118; 5-9ft 0/65; 1-4ft 7/100 • When children incur fatal injuries in falls of < 4ft, the history is incorrect. • The mortality of childhood falls. J Trauma. 1989; 29:1273-1275. • Fatalities: ≥ 50ft 8; 4-40ft 18; ≤ 3ft 18 • Minor falls can be lethal, especially in a toddler. • Additionally, we have found (as others) that it is extremely rare to have visceral, thoracic, or non-skull fractures in children who fall from < 3 floors. --if these injuries are found,one should suspect abuse.
Free Falls & Fatality • The nature of injuries associated with free falls in children is considerably different from that in adults. • Children <3 yrs are much less likely to have serious injuries than older children who fall the same distance. • It is thought that because younger children have more fat and cartilage and less muscle mass than older children, they dissipate the energy transferred by the fall. • Young children who fell from <3 m sustained only minor injuries, such as contusions, abrasions, and lacerations.
Free Falls & Fatality • Fractures were the most common of their serious injuries, and the radius, ulna and femur were the most frequent sites. • Mortality rate increased in falls from ≥6 m. • Children with low-level falls had a similar risk for intracranial and abdominal injury as those who fell from greater heights. • 58,000 fall-related hospitalizations and the 130 deaths below the age of 15 are most often associated with falls >10 m.
Free Falls & Fatality • Nearly 3/4 of falls from heights in children are unintentional, and the circumstances of injury should always be investigated for inflicted trauma, especially in children <5 yrs). • “Children Can’t Fly” program • Legally requiring window guards in all family houses with children <10 yrs old. • Accidental falls decreased by 96% in 4 yrs. • 98 children were injured during a 3-yr period from 1997 to 1999 in Dallas, because of an injury-prone situation permitted by older building codes