Download
1 / 21
210 likes | 238 Views
FEVER AND SKIN RASH. DR M. YOUSRY ABDEL-MAWLA,MD. Zagazig Faculty of Medicine. INTRODUCTION. The differential diagnosis for febrile patients with a rash is extensive. Diseases that present with fever and rash are usually classified according to the morphology of the primary lesion.

E N D
FEVER AND SKIN RASH DR M. YOUSRY ABDEL-MAWLA,MD. Zagazig Faculty of Medicine
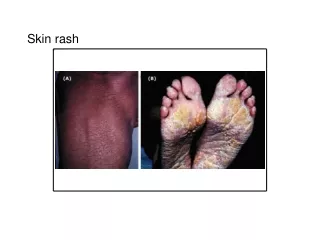
INTRODUCTION • The differential diagnosis for febrile patients with a rash is extensive. • Diseases that present with fever and rash are usually classified according to the morphology of the primary lesion.
MORPHOLOGIC CLASSIFICATION of RASH • Maculopapular . • Petechial. • Diffusely erythematous with desquamation. • Vesiculobullouspustular . • Nodular.
AETIOLOGICAL CLASSIFICATION • Viruses. • Bacteria. • Spirochetes. • Rickettsiae. • Medications • IMMUNOLOGIC-MEDIATED DISORDERS
HISTORY • A detailed history can be quite helpful in identifying the cause of fever and a rash. • A history of recent travel. • Animal exposure and inscet bites. • Drug ingestion • Contact with ill persons should be noted. • The time of year can be a clue to certain diagnoses • Any rash that is sudden in onset and covers a large part of the body • Any rash that starts either shortly after a flu-like illness begins, or a rash that starts after a flu-like illness goes away
Some disorders among travellers • Lyme disease. • Strongyloides stercoralis. • HIV/AIDS. • Rocky Mountain spotted fever. • Leishmaniasis. • Leprosy • STDs
Animal & Insect Contact Disorders • Animal contactQ fever.Anthrax.Viral hemorrhagic fevers.Cat scratch disease • Insect exposure: Mosquitoes:Malaria.Dengue. FilariasisYellow fever. Ticks :Tick typhus . Rocky Mountain spotted fever Lyme disease . Sand flies :Leishmaniasis&Sandfly fever Black flies :Onchocerciasis
Speacial care to the following • Conditions associated with valvular heart disease, • Sexually transmitted diseases or • Immunosuppression from chemotherapy. • Immune status is particularly important because many of the diseases that result in fever and a rash present differently in immunocompromised patients.
Details about the rash : • Site of onset, • Rate . • Direction of spread, • Presence or absence of pruritus. • Temporal relationship of rash and fever. • It is also important to know whether any topical or oral therapies have been attempted.
MACULE • Circumscribed area of change in normal skin color, with no skin elevation or depression; may be any size
PAPULE • Solid, raised lesion up to 0.5 cm in greatest diameter
NODULE • Similar to papule but located deeper in the dermis or subcutaneous tissue; differentiated from papule by palpability and depth, rather than size
PLAQUE • Elevation of skin occupying a relatively large area in relation to height; often formed by confluence of papules
VESICLE • Circumscribed, elevated, fluid-containing lesion less than 0.5 cm in greatest diameter; may be intraepidermal or subepidermal in origin
BULLA • Same as vesicle, except lesion is more than 0.5 cm in greatest diameter
LOOK FOR • The patient's vital signs and general appearance. • Signs of toxicity. • Adenopathy. • Oral, genital or conjunctival lesions. • Hepatosplenomegaly. • ]Evidence of excoriations or tenderness. • Signs of neck rigidity or neurologic dysfunction.
LABORATORY DATA The complete blood count with differential, an erythrocyte sedimentation rate, A chemistry panel, liver function tests. Blood and urine cultures Aspirates, scrapings and pustular fluid may be obtained for Gram staining and culture. Tzanck test may : unroofing a lesion and taking a scraping of the lesion base. Biopsy samples : from nonhealing or persistent purpuric lesions. Biopsy of inflammatory dermal nodules and ulcers
Specific diagnoses that may be confirmed histologically • Rocky Mountain spotted fever, herpetic infections, systemic lupus erythematosus, erythema multiforme, allergic vasculitis, secondary syphilis and deep fungal infections
Serologic tests • Systemic lupus erythematosus. • Other collagen vascular disorders • Syphilis. • Rheumatoid arthritis . • Human immunodeficiency virus infection.
Interesting, right? This is just a sneak preview of the full presentation. We hope you like it! To see the rest of it, just click here to view it in full on PowerShow.com. Then, if you’d like, you can also log in to PowerShow.com to download the entire presentation for free.