Download
1 / 105
1.05k likes | 2.2k Views
Seborrheic Dermatitis, Psoriasis, Recalcitrant Palmoplantar Eruptions, Pustular Dermatitis, and Erythroderma. P214-239 ANDREWS’ DISEASES OF THE SKIN. Seborrheic dermatitis. 2- 5 % of the population Chronic, superficial, inflammatory disease of the skin

E N D
Seborrheic Dermatitis, Psoriasis, Recalcitrant Palmoplantar Eruptions, Pustular Dermatitis, and Erythroderma P214-239 ANDREWS’ DISEASES OF THE SKIN
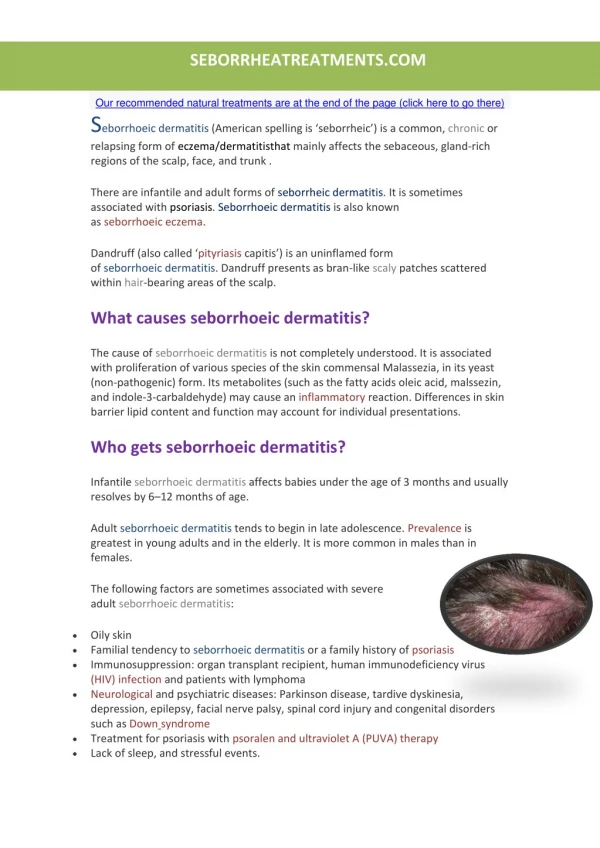
Seborrheic dermatitis • 2- 5 % of the population • Chronic, superficial, inflammatory disease of the skin • Predilection for the scalp, eyebrows, eyelids, nasolabial creases, lips, ears, sternal area, axillae, submammary folds, umbilicus, groin, and gluteal crease • Characterized by scanty, loose, dry, moist, or greasy scales, and by crusted pink or yellowish patches of various shapes and sizes
Clinical features • Remissions and exacerbations • No to mild itching • On the scalp is the most common • Pityriasis steatoides – oily type, accompanied by erythema and accumulation of thick crust • Frequently spreads beyond the scalp
Extreme cases involve the entire scalp and may have an offensive odor • Cradle cap • Marginal blepharitis – edges of the lids becoming erythematous and granular. Conjunctiva may be injected • On and in the ears may be mistaken for otitis externa caused by a fungal infection • KOH –
The presternal area is a favored site on the trunk • Common in the groin and the gluteal crease • In acute stages the inflammation may be intense, with moist exudation from the scalp and ears and papulovesicles on the palms and soles. Secondary infections, impetiginization, or furunculosis may ensue
May progress to a generalized exfoliative state • In the newborn this type of severe and generalized seborrheic dermatitis is known as erythroderma desquamativum • May be associated with or accentuated by several internal diseases • Parkinson’s, HIV, DM,
Etiology and pathogenesis • Remains unresolved • Presence of lipophilic yeast Pityrosporum ovale in large numbers in scalp lesion • Also demonstrated in those without seborrheic dermatitis • Healthy individuals have been found to have higher IgG antibodies to the organism
The significance of P ovale in infantile seborrheic dermatitis has not been fully evaluated • Familial tendency toward infantile and adult seborrheic dermatitis
histology • Epidermis is acanthotic • There is overlying focal scale crust often adjacent to follicular ostia • Slight spongiosis • Dermis contains a perivascular mixed cell inflammatory infiltrate
Differential diagnosis • Psoriasis, heavier scale and erythema, Auspitz’s sign, resistance to treatment, nail involvement • Crusted scabies of the scalp in immunodeficiency syndromes • Otitis externa, blepharitis, tinea corporis, pityriasis rosea, keratosis lichenoides chronica
Treatment • Selenium sulfide, tar, zinc, pyrithionate, resorcin shampoos • Nizoral • Corticosteroid solution • Antimicrobial preparations may be necessary • Bifonazole shampoo has been shown effective in treating infants and small children
Cortisporin otic usually brings about prompt clearing • Desonide Otic Lotion, 0.05% Desonide and 2% acidic acid is also effective • Topical steroids should not be used for blepharitis, since steroid preparations used in area may induce glaucoma and cataracts
psoriasis • A common, chronic, recurrent, inflammatory disease of the skin characterized by round, circumscribed, erythematous, dry, scaling plaques of various sizes, covered by grayish white or silvery white, imbricated and lamellar scales • Predilection for the scalp, nails, extensor surfaces, elbows, knees, umbilical, and sacral region
Typically symmetrical • May be a solitary macule to more than 100 • Usually develops slowly but may be exanthematous, with a sudden onset of numerous guttate lesions • Subjective symptoms such as itching or burning may be present and cause extreme discomfort
Scales are micaceous • Auspitz’s sign may be observed • Annular, lobulated, and gyrate figures may be produced • Old patches may be thickened and tough, and covered with lamellar scales like the outside of an oyster shell – psoriasis ostracea
Various other descriptive terms • Psoriasis guttata • Psoriasis follicularis • Psoriasis figurata, psoriasis annulata, psoriasis gyrata • Psoriasis discoidea • Psoriasis rupioides • Plaque psoriasis
Seborrheic-like psoriasis • In some cases of psoriasis prominent features of seborrheic dermatitis may occur not only if the typical sites of psoriasis vulgaris but also in the flexural areas such as the antecubital areas, axillae, under the breasts, groins, umbilicus, and intergluteal areas • Sebopsoriasis or seborrheic psoriasis
Inverse psoriasis • Flexural psoriasis or volar psoriasis • Selectively and almost exclusively involves folds, recesses, and flexural surfaces • Scalp quite often participates as well • Onycholysis, “Oil spots”, and nail pitting may be seen
“Napkin” psoriasis • Diaper dermatitis caused by the irritative effects of urine in the wet diaper area, may imitate a psoriasiform eruption • In addition there is commonly an infection with Candida albicans • Lesions typically clear • Infants may be at risk for psoriasis in adulthood
Psoriatic arthritis • The incidence of psoriasis is 10 times greater in persons with seronegative arthritis than in persons without arthritis
Five clinical patterns • Asymmetrical distal interphalangeal joint involvement with nail damage, 16% • Arthritis mutilans with osteolysis of phalanges and metacarpals, 5% • Symmetrical polyarthritis-like rheumatoid arthritis, with claw hands, 15% • Oligoarthritis with swelling and tenosynovitis of one or a few hand joints, 70% • Ankylosing spondylitis alone or with peripheral arthritis, 5%
Radiographic findings suggestive of psoriatic arthritis include: erosion of terminal phalangeal tufts, tapering of phalanges or metacarpals, “cupping’ of proximal ends of phalanges, , bony ankylosis, osteolysis of metatarsals, predilection for distal and proximal interphalangeal joints, paravertebral ossification, asymmetrical sacroiliitis, and rarity of “bamboo spine”when the spine is involved • Nearly half the patients with psoriatic arthritis have HLA-B27
Rest, splinting, passive motion, and aspirin or NSAIDs are appropriate • Methotrexate, cyclosporine, oral retinoids, sulfasalazine, tacrolimus, and PUVA are all likely to help both the psoriasis and arthritis • Systemic steroids however, the long term complications and potential for rebound in cutaneous disease restricts their use
Guttate psoriasis • This distinctive form of psoriasis typical lesions are the size of water drops • Usually occurs as an abrupt eruption following some acute infection, such as streptococcal pharyngitis • Occurs mostly in patients under age 30 • Recurrent episodes are likely, because of pharyngeal carriage of the responsible streptococcus • This type of psoriasis is usually rapidly responsive to topical steroids or UVB
Generalized pustular psoriasis(von Zumbusch) • Typical patients have had plaque psoriasis and often psoriatic arthritis • The onset is sudden, with formation of lakes of pus periungally, on the palms, and at the edge of psoriatic plaques • Pruritis and intense burning cause extreme discomfort • There is a fever, and a fetid odor develops • The pustules dry up to form yellow-brown crusts over a reddish-brown shiny surface
Generalized pustular psoriasis(von Zumbusch) • Mucous membrane lesions are common on the tongue and in the mouth • The lips are red and scaly, and superficial ulcerations of the tongue and mouth occur • May go through several stages • A number of cases of acute respiratory distress syndrome associated with pustular and erythrodermic psoriasis have been reported • Systemic complications include pneumonia, CHF and hepatitis
Generalized pustular psoriasis(von Zumbusch) • Etiology unclear • Iodides, coal tar, steroid withdrawal, terbinafine, minocycline, hydroxychloroquine, acetazolamide, and salicylates may trigger the attacks • May occur in infants • Acitretin is drug of choice, with a rapid and predictable response • Isotretinoin, cyclosporine, methotrexate, dapsone
course • The course of psoriasis is unpredictable • Usually begins on the scalp or elbows • May first be seen over the sacrum • Onset may be sudden and widespread • First lesions may be limited to the fingernails • Two of the chief features of psoriasis are its tendency to recur and persist
However, patients may remain completely free of lesions for years • Koebner’s phenomenon – the appearance of typical lesions of psoriasis at sites of eve trivial injury • Auspitz’s sign – pinpoint bleeding when the psoriatic scale is forcibly removed, this occurs because of severe thinning of the epidermis over the tips of the dermal papilla • Woronoff ring – is concentric blanching of the erythematous skin at or near the periphery of the healing psoriatic plaque
On the scalp absence of itching or hair loss, marked predilection for frontal scalp margin, deep erythema, and resistance to effective therapy for seborrheic dermatitis all suggest psoriasis • The palms and soles are often, sometimes exclusively, affected • “flexural” or inverse psoriasis shows salmon-red, demarcated plaques that frequently become eczematized, moist and fissured
Numerous cases of psoriasis of the mucous membranes have been reported • Fingernails and toenails may be involved. Characteristic changes include pits, onycholysis and cracking of the free edges • Many studies report an association of hepatitis C and psoriasis • Hepatitis C has also been implicated in psoriatic arthritis
etiology • The cause of psoriasis is still unknown • Heredity is of significance in some cases • Evidence that susceptibility to psoriasis is linked to class I and II major histocompatibility complex on human chromosome 6 (17q) • HLA associations include -Cw6, -B57, and -DR7 for early onset and -Cw2 for late onset psoriasis
It is believed also that any individual that has –B13 or –B17 has a fivefold risk of developing psoriasis • In pustular psoriasis HLA-B27 may be seen • -B13 and -B17 are increased in guttate and erythrodermic psoriasis
epidemiology • Equal frequency in both sexes • Mean age of onset is 27 years, range is wide • Sunlight improves • Emotional stress aggravates • 39% of patients experience complete periodic disappearance of psoriasis during its course • Seen in 1-2% of US population. Not seen in Native Americans
Distinct tendency to improvement with pregnancy • Exacerbation is common after childbirth
pathogenesis • Characterized by three main pathogenic features: abnormal differentiation, keratinocyte hyperproliferation and inflammation • Accelerated epidermopoiesis has been considered to be the fundamental pathologic event in psoriasis • The transit rate of psoriatic keratinocytes is increased, and the deoxyribonucleic acid synthesis time is decreased
Early lesion are infiltrated predominantly by lymphocytes in the papillary dermis • The cause of T-lymphocyte activation and the role of these cell populations remains unclear
stress • Studies have shown a positive correlation between stress and the severity of disease
Drug-induced psoriasis • May be induced by many drugs: beta blockers, lithium, and antimalarials, terbinafine, calcium channel blockers, captopril, glyburide, and lipid lowering agents such as gemfibrozil
Pathology • Regular epidermal hyperplasia with long, test-tube-shaped rete ridges • Thinning of dermal papillae • Granular layer is thin or absent • Overlying parakeratosis • Small collections of neutrophils (Munro microabcesses) may be present in the stratum corneum • There is a perivascular mononuclear cell infiltrate
Differential diagnosis • Seborrheic dermatitis, pityriasis rosea, lichen planus, eczema, psoriasiform syphilid, and lupus erythematosis • Distribution, quality of the scale and presence of Auspitz’s sign, symptoms, serologic testing