Download
1 / 38
380 likes | 478 Views
An Overview of Disparities and Improving the Collection of Race, Ethnicity, and Language Data: the MDPH Approach NAPHSIS ANNUAL MEETING, 2007. Bruce B. Cohen and Brunilda Torres Massachusetts Department of Public Health June 2007. Overview: Improving Data Collection. Historical Context

E N D
An Overview of Disparities and Improving the Collection of Race, Ethnicity, and Language Data: the MDPH ApproachNAPHSIS ANNUAL MEETING, 2007 Bruce B. Cohen and Brunilda Torres Massachusetts Department of Public Health June 2007
Overview: Improving Data Collection • Historical Context • History of MDPH efforts • Need for more detailed data • Defining principles • Proposed questions
OMB Standards Office of Management and Budget Directive 15 issued in 1977 set standards • revised in 1997 • sets minimum standards for the collection of race and ethnicity data for all federal data sets • all current surveys should have complied with the 1997 revision by January 1, 2003
OMB 1997 revision • Major changes • when self identification is used, • a method for reporting more than one race should be adopted • this method should NOT be a “multiracial” category, but rather a multiple response to a single question • a two question format should be used, with the Hispanic origin question preceding the race question
OMB 1997 revision Major changes (continued) • when self identification is NOT used (ie. observer, proxy or record based) • a method for reporting more than one race should be adopted • this method should NOT be a “multiracial” category, but rather a multiple response to a single question • a two question format should be used, with the Hispanic origin question preceding the race question • a one question format may be used, with “Hispanic” as a race category
1997 white black or African American American Indian or Alaska Native Asian Native Hawaiian or Other Pacific Islander NOTE: Only the US Census Bureau for the purpose of the Census 2000 and NCHS for the revised standard certificates of birth and death have been granted variances to include an “other” category 1977 white black American Indian Asian or Pacific Islander OMB Revised Race Categories
Census 2000: Ethnicity Question(ADOPTED by NCHS in Revised Certificate) • Is person 1 Spanish/Hispanic/Latino? Mark x in the “No” box if not Spanish/Hispanic/Latino. • No, not Spanish/Hispanic/Latino • Yes, Mexican, Mexican Am., Chicano • Yes, Puerto Rican • Yes, Cuban • Yes, other Spanish/Hispanic Latino- print group.
Census 2000: Race questionAdopted by NCHS What is Person 1’s race? Mark x in one or more races White Black, African American or Negro American Indian or Alaskan Native- print name of enrolled or principal tribe Asian IndianNative Hawaiian ChineseGuamanian or Chamorro FilipinoSamoan Japanese Other Pacific Islander- print race Korean Some other race- print race Vietnamese Other Asian- print race
OMB in Historical Context OMB 15 in historical context Lessons for states in implementing OMB 15 • race categories changed regularly over time • race categories determined by social and cultural context • race categories will continue to be determined by and reflect social and cultural context • ethnicity and national origin categories • more stable over time • change to reflect changing demographics, not social and cultural context • highly salient to state and local public health practice
Impact of OMB and Federal and State Public Health Practice Purpose of data collection • state and federal similar: ongoing monitoring to identify priorities, program evaluation, and high need areas • state and federal differ: • state needs for service targeting to high risk individuals • state needs for service targeting to high risk communities
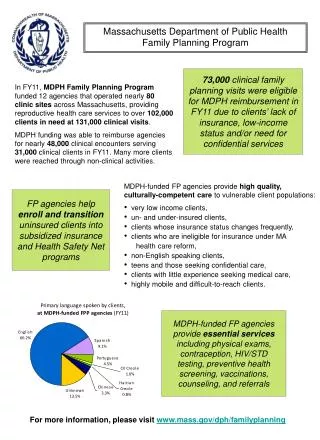
DPH efforts to date 1980-90’s: Special reports on disparities, e.g.: Black Men Endangered, Disparities Commission testimony, ongoing surveillance reports, detailed ethnicity perinatal reports 2000: Efforts to identify R/E/L methods in MDPH databases 2001: Collection of race/ethnicity and language required in hospital acute care settings as result of Interpreters’ Services Regulations 2002: Internal meetings to develop MDPH standards 2003: MDPH data standards committee review 2005: Collaboration with Boston Public Health Commission for consistent standards 2006: Joined with Division of Health Care Finance and Policy to promulgate case-mix data regulations implement 1/2007 for hospital discharge and emergency department data 2007: February, MDPH issues new standards
Breastfeeding among Mothers by Race Massachusetts: 2000-2004 Source: Massachusetts Births 2002-20044 *Non-Hispanic
Breastfeeding among Mothers by Ethnicity, MA:2000-2004 Blacks Hispanics Asians Source: MDPH, Center for Health Information, Statistics, Research & Evaluation, Research & Epidemiology Program
Cesarean Section Deliveries among Mothers by Race, MA:2000-2004 Source: Massachusetts Births 2002-20044 *Non-Hispanic
Mother’s Ethnicity and Cesarean Rates All Deliveries* MA 2004 * A delivery of multiples is counted once Source: Massachusetts Births 2004
MDPH Proposal • Collect Hispanic ancestry and race categories consistent with Federal OMB standards • Expand collection to include detailed ethnicity data • Collect language data consistent with LEP (Limited English Proficiency) guidance issued by DHSS in 2002
Principles for Data Collection • Encourage client self-report • Allow for the selection of multiple categories • Collect information on detailed ethnicity groups as well as broad race categories • Incorporate language preference as basic sociodemographic characteristic • Maintain consistency with Federal OMB standards
Basic concepts Race: group or groups that an individual identifies with because they share similar physical characteristics or social and geographic origins. Ethnicity: a person’s background, heritage, culture, ancestry, country of birth
OF RACE monitors discrimination, yields more stable rates Follows OMB standard more routinely collected OF ETHNICITY better understood less context dependent more useful for program targeting and development improved sensitivity to linguistic needs added insight into acculturation Added Value
WITH RACE changing over time not clearly understood conceptually context dependent heterogeneity within groups used as proxy WITH ETHNICITY lack of denominators for population based rates small numbers for analysis requires more complex data collection more variable by geography Concerns
Advantages client centered care target interventions monitor demographic change health status monitoring Disadvantages expanded IT efforts moves beyond Federal minimum standards lack of denominator data for calculating rates increases data collector and respondent burden Collecting Both
Proposed New Questions • 5-Question Format • Define a Minimum set of categories • Allow for expansion to meet local needs • Allows for free text • Maintain consistency with Federal standards
Question 1 1. Are you Hispanic/Latino/Spanish? ❑ Yes ❑ No
Question 3, Race • What is your race? (You can specify one or more) ❑ American Indian/Alaska Native (specify tribal nation___________________) ❑ Asian ❑ Black ❑ Native Hawaiian or other Pacific Islander (specify) ❑ White ❑ Other (specify ___________________) ❑ Unknown/not specified
Questions 4 and 5: Language Preference 4. In what language do you prefer to discuss health-related concerns? ❑ Albanian ❑ Portuguese ❑ Arabic ❑ Russian ❑ Cape Verdean Creole ❑ Somali ❑ Chinese (specify) ❑ Spanish ❑ English❑ Vietnamese ❑ Haitian Creole ❑ Other (specify) ❑ Khmer 5. In what language do you prefer to read health-related materials?_____________
Keys to successful implementation • Making the data collector comfortable • Making the respondent comfortable • Helping the respondent understand the importance of the information
Field Testing and Training • ~ 9000 patients • ~1,200 WIC participants • Four statewide “Train the Trainer” training sessions for 200 hospital personnel
Current Status • DHCFP -- Implementation 1/2007 • BPHC --Implementation 7/2007 • MDPH – Implementation ongoing • Support via BPHC, DHCFP, MHA – Ongoing http://www.mhalink.org/
Lessons learned • Overall, data collectors and program participants feel very favorably about this process. • Training of data collectors is crucial: • Purpose and importance of data • Strategies for using new data • Strategies for answering common questions; • Need to reach out to our community partners • Need to bring IT into this process