Download
1 / 1
10 likes | 151 Views
Complications Associated with Ceramic vs. Titanium Halo Pins: A Retrospective Review. Megan Zachar CO, Molly Hill MSPO, Sara Pschigoda CO, Jeffrey Wensman CPO, Gregory Graziano MD, Rakesh Patel MD, Claire Kalpakjian PhD. Introduction & Purpose. Methods. Discussion. Results.

E N D
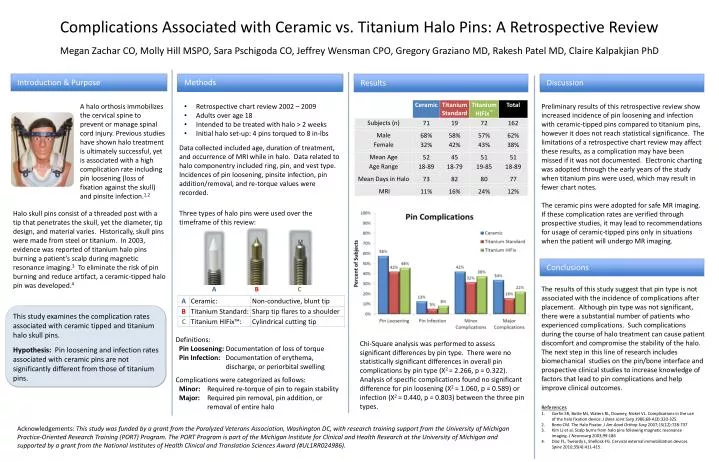
Complications Associated with Ceramic vs. Titanium Halo Pins: A Retrospective Review Megan Zachar CO, Molly Hill MSPO, Sara Pschigoda CO, Jeffrey Wensman CPO, Gregory Graziano MD, Rakesh Patel MD, Claire Kalpakjian PhD Introduction & Purpose Methods Discussion Results A halo orthosis immobilizes the cervical spine to prevent or manage spinal cord injury. Previous studies have shown halo treatment is ultimately successful, yet is associated with a high complication rate including pin loosening (loss of fixation against the skull) and pinsiteinfection.1,2 Preliminary results of this retrospective review show increased incidence of pin loosening and infection with ceramic-tipped pins compared to titanium pins, however it does not reach statistical significance. The limitations of a retrospective chart review may affect these results, as a complication may have been missed if it was not documented. Electronic charting was adopted through the early years of the study when titanium pins were used, which may result in fewer chart notes. The ceramic pins were adopted for safe MR imaging. If these complication rates are verified through prospective studies, it may lead to recommendations for usage of ceramic-tipped pins only in situations when the patient will undergo MR imaging. • Retrospective chart review 2002 – 2009 • Adults over age 18 • Intended to be treated with halo > 2 weeks • Initial halo set-up: 4 pins torqued to 8 in-lbs • Data collected included age, duration of treatment, and occurrence of MRI while in halo. Data related to halo componentry included ring, pin, and vest type. Incidences of pin loosening, pinsite infection, pin addition/removal, and re-torque values were recorded. Halo skull pins consist of a threaded post with a tip that penetrates the skull, yet the diameter, tip design, and material varies. Historically, skull pins were made from steel or titanium. In 2003, evidence was reported of titanium halo pins burning a patient’s scalp during magnetic resonance imaging.3 To eliminate the risk of pin burning and reduce artifact, a ceramic-tipped halo pin was developed.4 This study examines the complication rates associated with ceramic tipped and titanium halo skull pins. Hypothesis: Pin loosening and infection rates associated with ceramic pins are not significantly different from those of titanium pins. Three types of halo pins were used over the timeframe of this review: Conclusions The results of this study suggest that pin type is not associated with the incidence of complications after placement. Although pin type was not significant, there were a substantial number of patients who experienced complications. Such complications during the course of halo treatment can cause patient discomfort and compromise the stability of the halo. The next step in this line of research includes biomechanical studies on the pin/bone interface and prospective clinical studies to increase knowledge of factors that lead to pin complications and help improve clinical outcomes. ABC • Definitions: • Pin Loosening: Documentation of loss of torque • Pin Infection: Documentation of erythema, discharge, or periorbitalswelling • Complications were categorized as follows: • Minor: Required re-torque of pin to regain stability • Major: Required pin removal, pin addition, or removal of entire halo Chi-Square analysis was performed to assess significant differences by pin type. There were no statistically significant differences in overall pin complications by pin type (Χ2 = 2.266, p = 0.322). Analysis of specific complications found no significant difference for pin loosening (X2 = 1.060, p = 0.589) or infection (X2 = 0.440, p = 0.803) between the three pin types. • References • GarfinSR, Botte MJ, Waters RL, Downey, Nickel VL. Complications in the use of the halo fixation device. J Bone Joint Surg 1986;68-A(3):320-325. • Bono CM. The Halo Fixator. J Am AcadOrthopSurg 2007;15(12):728-737. • Kim LJ et al. Scalp burns from halo pins following magnetic resonance imaging. J Neurosurg2003;99:186 • Diaz FL, Tweardy L, Shellock FG. Cervical external immobilization devices Spine2010;35(4):411-415. Acknowledgements: This study was funded by a grant from the Paralyzed Veterans Association, Washington DC, with research training support from the University of Michigan Practice-Oriented Research Training (PORT) Program. The PORT Program is part of the Michigan Institute for Clinical and Health Research at the University of Michigan and supported by a grant from the National Institutes of Health Clinical and Translation Sciences Award (#UL1RR024986).