Download
1 / 85
940 likes | 1.28k Views
VENOUS THROMBOEMBOLISM PROPHYLAXIS for the Hospitalized Medical Patients. Madel Sadili, MD, FCCP, FPCCP. Lecture Outline. Arterial & Venous Thrombosis Burden Of Disease (VTE) Incidence Rationale for Thromboprophylaxis Risk Factors Grading of Recommendations Recommendations

E N D
VENOUSTHROMBOEMBOLISMPROPHYLAXISfor the Hospitalized Medical Patients Madel Sadili, MD, FCCP, FPCCP
Lecture Outline • Arterial & Venous Thrombosis • Burden Of Disease (VTE) • Incidence • Rationale for Thromboprophylaxis • Risk Factors • Grading of Recommendations • Recommendations • Drugs • Summary
Lecture Outline • Arterial & Venous Thrombosis • Burden Of Disease (VTE) • Incidence • Rationale for Thromboprophylaxis • Risk Factors • Grading of Recommendations • Recommendations • Drugs • Summary
Venous Thromboembolism(VTE) • DVT : Deep-vein thrombosis • PE : Pulmonary Embolism
Arterial Thrombosis • Most common cause of MI, stroke, & limb gangrene • Usually is initiated by the spontaneous or mechanical rupture of atherosclerotic plaque • Consists of platelet aggregates held together by small amounts of fibrin • Strategies to inhibit arterial thrombogenesis focus mainly on drugs that block platelet function but often include anticoagulant agents to prevent fibrin deposition
Venous thrombosis • Leads to PE (can be fatal) & to postphlebitic syndrome • Occurs when procoagulant stimuli overwhelm natural protective mechanisms, ie, excessive activation of coagulation with thrombophilic abnormalities, vessel wall damage or stasis; inflammatory cytokines generated after trauma, surgery, or medical illness activate endothelial cells that express adhesion molecules that attract leukocytes which elaborate tissue factor & express receptors for factor X & fibrinogen, that promotes coagulation on their surfaces; neutrophils generate O2 free radicals & release hydrolytic enzymes, enhancing local clot formation • Venous thrombus is composed mainly of fibrin & RBCs • Anticoagulants are the drugs of choice for their prevention & treatment
Lecture Outline • Arterial & Venous Thrombosis • Burden Of Disease (VTE) • Incidence • Rationale for Thromboprophylaxis • Risk Factors • Grading of Recommendations • Recommendations • Drugs • Summary
Hospitalization for an acute medical illness • Independently associated with ~8fold increase in relative risk for VTE (Heit, et al. Arch Int Med 2000;160) • 10-30% of general medical patients may develop VTE (Cohen, et al. Thromb Haemost 2005; 94) • 50-70% of symptomatic thromboembolic events, and 70-80% of fatal PEs occur in non-surgical patients (Goldhaber, et al. Chest 2000; 118) • ¾ of VTE in hospitalized patients occur in acutely ill nonsurgical patients (Leizorovicz, et al. J Thrombosis & Hemostasis 2003)
PE (postmortem studies) is associated with up to 10% of deaths in hospitalized patients, and only ¼ of these occur following surgery thus… ¾ of hospitalized patients who suffer a fatal PE are in fact medical patients Cohen et al. Thromb Haemost 2005; 94
VTE: Magnitude of the Problem DVT 2 million cases PE 600,000 cases Post-thrombotic syndrome 800,000 cases Death 60,000 cases Pulmonary hypertension 30,000 cases Estimated cost of VTE care = US$ 1.5 billion/year Goldhaber SZ et al. Lancet 1999;353:1386–9
Therefore... the appropriate prophylaxis of medical inpatients offers an important opportunity to significantly reduce the burden of disease due to VTE
Lecture Outline • Arterial & Venous Thrombosis • Burden Of Disease (VTE) • Incidence • Rationale for Thromboprophylaxis • Risk Factors • Grading of Recommendations • Recommendations • Drugs • Summary
Rationale High Prevalence of VTE Adverse Consequences of unprevented VTE Efficacy & Effectiveness of thromboprophylaxis Description Most hospitalized px have risk factors for VTE DVT is common in many hospitalized px Hosp-acquired DVT & PE are usually clinically silent Difficult to predict which at-risk patients will develop symptomatic thromboembolic complications Screening at-risk px using PE or noninvasive testing is neither effective nor cost-effective Symptomatic DVT & PE Fatal PE Costs of investigating symptomatic patients Risks & costs of treating unprevented VTE, esp bleeding Increased future risk of recurrent VTE Chronic post-thrombotic syndrome Thromboprophylaxis is highly efficacious at preventing DVT, proximal DVT, symptomatic VTE, & fatal PE Prevention of DVT also prevents PE Cost-effectiveness of prophylaxis has repeatedly been demonstrated Geerts, et al. Chest 2001; 119:132S-175S
Lecture Outline • Arterial & Venous Thrombosis • Burden Of Disease (VTE) • Incidence • Rationale for Thromboprophylaxis • Risk Factors • Grading of Recommendations • Recommendations • Drugs • Summary
Surgery • Trauma (major or lower extremity) • Immobility, paresis • Malignancy • Cancer therapy (hormonal, chemotx, radiotx) • Previous VTE • Increasing age • Pregnancy & the postpartum period • Estrogen-containing oral contraception or HRT • Selective estrogen receptor modulators • Acute medical illness • Heart or respiratory failure • Inflammatory bowel disease • Nephrotic syndrome • Myeloproliferative disease • Paroxysmal nocturnal hemoglobinuria • Obesity • Smoking • Varicose veins • Central venous catheterization • Inherited or acquired thrombophilia Heit, et al. Arch Int Med 2002; 162:1245-1248
Absolute risk of DVT in Hospitalized Patients • Medical px10-20 % • General surgery 15-40 • Major gyne surgery 15-40 • Major urologic surgery 15-40 • Neurosurgery 15-40 • Stroke20-50 • Hip or knee arthroplasty; hip fracture surgery 40-60 • Major trauma 40-80 • Spinal cord injury 60-80 • Critical care patients10-80 Geerts, et al. Chest 2001; 119:132S-175S
Despite consensus-group recommendations that at-risk medical patients should receive thromboprophylaxis, there is NO CONSENSUS as to which patients are at risk, thus, many patients may not receive appropriate thromboprophylaxis Cohen, et al. Thromb Haemost 2005: 94
Thromboprophylaxis in Acutely Ill Patients MEDENOX (1999) Prophylaxis of VTE in MEDical Patients with ENOXaparin • 40mg, 20mg enoxaparin vs placebo OD x 6-14 days • 866 patients with heart failure, respiratory, & infectious disease • Primary outcome – VTE between days 1-14 – DVT detected by bilateral venography (or duplex utz) between days 6-14 (or earlier if clinically indicated) or documented PE • Duration of ff-up – 3 months Samama MM et al. N Engl J Med 1999;341:793–800
MEDENOX: Incidence of VTE at Day 14 P = 0.0002 RRR = -63% P = 0.037 RRR = -65% NS NS = not significant Samama MM et al. N Engl J Med 1999;341:793–800
MEDENOX • The incidence of VTE was significantly lower in the 40mg enoxaparin group (5.5%) than in the placebo (14.9%) • The benefit was maintained at 3 months
PREVENT (2003) • Prospective evaluation of Dalteparin efficacy for the prevention of VTE in immobilized patients • Largest trial (radomized, double-blind, palacebo-controlled) comparing a LMWH with placebo – Dalteparin 5000 IU OD x 14 days • 3706 acutely ill medical patients – CHF, acute respiratory failure, or infectious disease • Primary endpoint – clinically important VTE defined as objectively verified symptomatic DVT, PE, sudden death, & objectively verified asymptomatic proximal DVT. Compression UTZ done in all patients who had not reached an endpoint by day 21 Leizorovicz, et al. J Thrombosis & Haemostasis. July 2003
PREVENT: Results P=0.0015 • Medically ill patients • 52% CHF • 30% respiratory failure • Also, infection without septic shock, rheumatic disorders, arthritis of the legs, or inflammatory bowel disease Leizorovicz A. et al J Thromb Haemost 2003; 1 (Suppl 1):)OC396
PREVENT • The incidence of the composite primary outcome was 2.77% in the dalteparin group and 4.96% in the placebo group, a risk reduction of 45%
Lecture Outline • Arterial & Venous Thrombosis • Burden Of Disease (VTE) • Incidence • Rationale for Thromboprophylaxis • Risk Factors • Grading of Recommendations • Recommendations • Drugs • Summary
Lecture Outline • Arterial & Venous Thrombosis • Burden Of Disease (VTE) • Incidence • Rationale for Thromboprophylaxis • Risk Factors • Grading of Recommendations • Recommendations • Drugs • Summary
Recommendations: Thromboprophylaxis in the Medically Ill Geerts, et al. Chest Supplement. Sept 2004; 126/3
General Recommendations • It is recommended that mechanical methods of prophylaxis be used primarily in patients who are at high risk of bleeding (Grade 1C+) or as an adjunct to anticoagulant-based prophylaxis (Grade 2A). Careful attention should be directed toward ensuring the proper use of, and optimal compliance with, the mechanical device (Grade 1C+) • We recommend against the use of aspirin alone as prophylaxis against VTE for any patient group (Grade 1A) • For each of the antithrombotic agents, it is recommended that clinicians consider the manufacturer’s suggested dosing guidelines (Grade 1C)
General Recommendations • We recommend consideration of renal impairment when deciding on doses of LMWH, fondaparinux, the direct thrombin inhibitors, & other antithrombotic drugs that are cleared by the kidneys, particularly in elderly patients and those who are at high risk for bleeding (Grade 1C+) • In all patients undergoing neuraxial anesthesia or analgesia, special caution when using anticoagulant prophylaxis is recommended (Grade 1C+)
Medical Conditions • In acutely ill medical patients who have been admitted to the hospital with CHF or severe respiratory disease, or who are confined to bed & have 1 or more additional risk factors, including active cancer , previous VTE, sepsis, acute neurologic disease, or inflammatory bowel disease, prophylaxis with LDUH or LMWH is recommended (Grade IA) • In medical patients with risk factors for VTE, & in whom there is a contraindication to anticoagulant prophylaxis, the use of mechanical prophylaxis with GCS or IPC is recommended (Grade 1C+)
Medical Condition: Acute MI • For all patients at high risk of systemic or venous thromboembolism (anterior MI, pump failure, previous embolus, atrial fibrillation, or LV thrombus), the administration of IV UFH while receiving streptokinase, is recommended (Grade 1C+)
Medical Condition: Acute Ischemic Stroke • For acute stroke patients with restricted mobility, prophylactic low-dose subcutaneous heparin or LMWH or heparinoids is recommended (Grade 1A). *Low-dose heparin should be restricted for 24h after administration of thrombolytic therapy; it may be used safely in combination with aspirin. • For patients who have contraindications to anticoagulants, it is recommended that clinicians use intermittent pneumatic compression devices or elastic stockings (Grade 1C)
Medical Conditions: Intracerebral Hemorrhage • We recommend the initial use of intermittent pnuematic compression (Grade 1C+). • In stable patients, low-dose SQ heparin may be initiated as soon as the 2nd day after the onset of the hemorrhage (Grade 2C). Underlying values and preferences: the recommendation for SQ heparin assumes a relatively low degree of risk aversion.
Cancer Patients • 6-fold increased risk of VTE compared to those without cancer • More specific risk estimates of VTE by cancer type, stage, and treatment approaches are still largely unknown • High among those with malignant brain tumors and adenocarcinoma of the ovary, pancreas, colon, stomach, lung, prostate, and kidney • Cancer patients undergoing surgery have at least 2x the risk of postoperative DVT and more than 3x the risk of fatal PE
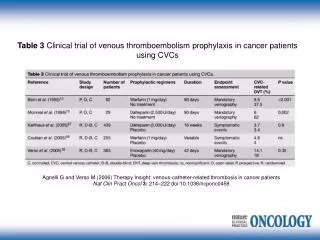
Cancer Patients • Cancer patients undergoing surgical procedures receive prophylaxis that is appropriate for their current risk state (Grade 1A). Refer to the surgical subsections. • Hospitalized cancer patients who are bedridden with an acute medical illness should receive prophylaxis that is appropriate for their current risk state (Grade 1A). Refer to the medical subsection. • It is suggested that clinicians not routinely use prophlaxis to try to prevent thrombosis related to long-term indwelling CVCs in cancer patients (Grade 2B).
Critical Care • On admission to a critical care unit, all patients should be assessed for their risk of VTE. Accordingly, most patients should receive thromboprophylaxis (Grade 1A) • For patients who are at high risk for bleeding, mechanical prophylaxis with GCS &/or IPC is recommended, until the bleeding risk decreases (Grade 1C+) • For ICU patients who are at moderate risk for VTE (eg, medically ill or postoperative px), LDUH or LMWH prophylaxis is recommended (Grade 1A) • For patients who are at higher risk, such as that following major trauma or orthopedic surgery, LMWH prophylaxis is recommended (Grade 1A)
BURNS • Burn patients with additional risk factors for VTE, including one or more of the ff: advanced age, morbid obesity, extensive or lower extremity burns, concomitant lower extremity trauma, use of a femoral venous catheter, &/or prolonged immobility (Grade 1C+) • If there are no contraindications, the use of either LDUH or LMWH is recommended, starting as soon as it is considered safe to do so (Grade 1C+)
Increased Risk of Bleeding • Recent surgery • Known bleeding disorder • Impaired renal function • Uncontrolled hypertension • Large ischaemic cerebral infarction • Active GI bleeding (peptic/bowel) • Use of antiplatelet drugs or NSAIDs
Lecture Outline • Arterial & Venous Thrombosis • Burden Of Disease (VTE) • Incidence • Rationale for Thromboprophylaxis • Risk Factors • Grading of Recommendations • Recommendations • Drugs • Summary
Methods of DVT Prophylaxis • Unfractionated heparin (UFH) • Low-molecular-weight heparins (LMWHs) • Oral anticoagulants (warfarin) • Pentasaccharides (fondaparinux) • Antiplatelet therapy • Mechanical compression and early ambulation
Unfractionated Heparin • Main anticoagulant action is mediated by the heparin/AT interaction, which inactivates thrombin factor IIa & factors Xa, IXa, & XIIa • Increases vessel wall permeability, suppresses proliferation of vascular smooth muscle cells, suppresses osteoblast formation, & activates osteoclasts, promoting bone loss, & HIT • IV infusion or SC injection (reduced bioavailabiltiy, thus, 10% higher initial dose) • Dose adjustment by monitoring aPTT, or, when very high doses are given, by ACT (activated clotting time)
LMWH • Polysulfated glycosaminoglycans about 1/3 the molecular weight of UFH • Like heparin, major anticoagulant effect by activating AT • Administered in fixed doses, for thromboprophylaxis, or in total body weight (TBW)-adjusted doses, for therapeutic effect
LMWH • Reduced binding properties to proteins & cells, explaining all of the anticoagulant, phramacokinetic, & other biological differences between heparin & LMWH: -reduced ability to inactivate thrombin bec the smaller fragments cannot bind simultaneously to AT & thrombin, but, since bridging bet AT & factor Xa is less critical for factor Xa activity, the smaller fragments inactivate factor Xa almost as well as larger molecules -reduced binding to plasma proteins is responsible for the more predictable dose-response relationship of LMWHs -lower binding to macrophages & endothelial cells increases the plasma half-life of LMWHs -reduced binding to platelets & PF4 explains lower incidence of HIT -reduced binding to osteoblasts results in lower incidence of bone loss
Fondaparinux • New parenteral indirect factor Xa inhibitor, with no activity against thrombin • Excellent bioavailability after SQ injection with a plasma half-life of 17h, thus given OD • Does not bind to platelets or PF4 (no heparin/PF4 complex), thus, no HIT • Phase III trial for thromboprophylaxis at 2.5mg OD