Download
1 / 16
160 likes | 162 Views
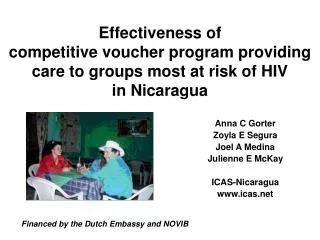
This study evaluates the effectiveness of a competitive voucher program in providing quality STI/HIV care to populations most at risk in Nicaragua. The program, financed by the Dutch Embassy and NOVIB, targets marginalized groups by distributing vouchers at prostitution sites and other gathering places. Results show significant reductions in STI prevalence and increases in condom use among sex workers. The program successfully attracts even the most marginalized individuals to high-quality care, contributing to the maintenance of low HIV prevalence in Nicaragua.

E N D
Anna C Gorter Zoyla E Segura Joel A Medina Julienne E McKay ICAS-Nicaragua www.icas.net Effectiveness of competitive voucher program providing care to groups most at risk of HIV in Nicaragua Financed by the Dutch Embassy and NOVIB
Background • HIV prevalence remains low in Nicaragua • Populations most at risk often receive inadequate STI/HIV care due to: • Costs of and distance to care • Marginalization, stigmatizing • Need for special measures, however • Quality STI/HIV care is expensive • Limited resources should betargeted
Competitive voucher schemes • Competitive voucher schemes can easilytarget limited resources to populations most at HIV-risk by distributing vouchers at prostitution sites or other sites where these groups congregate • Competitive vouchers are a type of demand side financing
Demand side financing compared to Supply side financing Demand Side Financing Supply Side Financing Competitive Vouchers Scheme Current System (Inputs) High Consumer empowerment Low Good Targeting Poor High Choice Low/No High Provider Competition Low/No
Providing groups most at risk with quality STI/HIV care • 1996: start competitive voucher program • Regular distribution vouchers(2-3x/year) • Contracting clinics on competitive basis • Clinics trainedin high efficacy treatment and ‘social’ protocols, closely monitored • Voucher recipients obtain free counselling, treatment/care at clinic of their choice
Voucher NGO's V O U C H E R V O U C H E R V O U C H E R Agency ICAS V O U C H E R V O U C H V E O R U C H E R Donor/ Government Groups most at risk of HIV Clinics V O U C H E R V Clients & O U C H Partners E R
Results 1996-2005 • >25 clinics contracted and trained in public, private, NGO sector • 160,000 field contacts with sex workers, glue-sniffers, transvestites, regular clients and MSM • 60,000 vouchers distributed in 21 rounds • 20,000 consultations • 7,000 STIs and 9,000 RTIs cured • 2,300 VCT (42 persons HIV positive:1.8%)
Results Managua 1996-2005 • We report results for 10,000 consultations provided to sex workers in Managua • Exogenous changes in frequency of voucher distribution rounds(see next slide), resulting from irregular financial flows, and with no changes in other possible explanators, allows to attribute observed STI reduction to program (published in AJPH 2006;96:7-9)
Reduction of syphilis and trichomonas in sex workers of Managua in 21 rounds of voucher distribution (1996-2005)
All SWs Managua Glue-sniffers Poor SW at Markets Bars/ Streets Red Light area Mean N of vouchers distributed 2-3 times per annum ‘96-‘05 1,100 75 335 490 200 Syphilis prevalence 1996 and 2005 9%-3%*** 28%-7%*** 17%-4%*** 6%-1%** 1%-0.5% Trichomonas prevalence 1996 and 2005 16%-8%*** 39%-15%** 13%-6%* 15%-7%** 10%-8% Condom use 2002 and 2005 51%-67%*** 39%-32% 47%-69%*** 55%-76%*** 61%-79%** Overview reduction syphilis and trichomonas and increase condom use among different socio-economic strata sex workers *P<0.05; **P<0.005; ***P<0.00001
Reduction syphilis in all socio-economic strata (especially in the poorest)
Reduction trichomonas in all socio-economic strata (especially poorest)
HIV prevalence: 1991: 0.8% 1996: 1.5% 1997: 1.3% 1999: 2.0% 2000: 0.9% 2003: 2.7% HIV prevalence sex workers Managua remained low, in marked contrast to other Central American countries Young sex workers in nightclub
Reaching groups most at risk with STI/HIV care successful • The voucher program: • attracted even most marginalized sex workers (SW) to high efficacy STI/HIV care • reduced STI prevalence / increased condom use • contributed to maintaining low HIV prevalence • SWs in lowest strata, with highest initial STI rates, recorded most significant declines
More information: www.icas.net anna@icas.net zoyla@icas.net