Download
1 / 16
240 likes | 565 Views
ACCOUNTABLE CARE ORGANIZATIONS (ACOs). Safiah Mamoon HTM 520. INTRODUCTION. U.S. healthcare sector– very large with fragmented care High spending for poor outcomes Care not coordinated Providers reimbursed for services regardless of quality According to the IOM, care needs to be: Safe

E N D
ACCOUNTABLE CARE ORGANIZATIONS(ACOs) Safiah Mamoon HTM 520
INTRODUCTION • U.S. healthcare sector– very large with fragmented care • High spending for poor outcomes • Care not coordinated • Providers reimbursed for services regardless of quality • According to the IOM, care needs to be: • Safe • Effective • Efficient • Equitable • Timely • Patient-centered
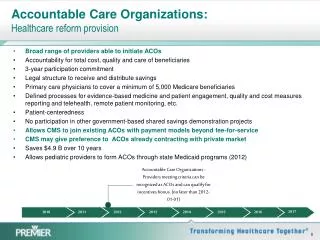
WHAT IS AN ACO ? • Set of providers jointly held accountable for • achieving measured quality improvements • reductions in the rate of spending growth • Provides coordinated, patient-centric services across continuum of care in designated population • Comprised of • primary care physicians • Specialists • hospitals • post-acute care facilities • health insurance plans • Other
ACA and ACO • ACA of 2010 required Medicare to start utilizing ACOs by 2012 • To participate in the Medicare Shared Savings Program (MSSP), ACO must • Enroll 5000 Medicare beneficiaries • Participate in the MSSP for a minimum of 3 years • Share in any cost savings that arise from quality improvements and enhanced efficiency
ACO and Meaningful Use (MU) • ACO need to show improved performance on 65 clinical measures in 3-year period • 26 of 65 requirements also MU Criteria captured by certified EHR system • Strong alignment between EHR incentive program and MSSP • MU and HIEs will help ACO meet many of its objectives
ACO AND MU • MU • Improve quality, safety, efficiency, and reduce health disparities • Engage patients and families • Improve care coordination • Ensure adequate privacy and security protections for personal health information • Improve population and public health. MU goals
ACOs and Quantifiable Data • Demonstrate evidence-based medical practice • Demonstrate patient engagement • Report on quality and cost measures • Demonstrate improved outcomes • Demonstrate cost-savings • Value-based reimbursement • Financial incentives
Organizations • AHIC
Barriers and Challenges • Financial • Business • HIE-related • Standards and Certification • Privacy and Security • Cultural • Legal
FUTURE TRENDS • December, 2013—500 ACOs • Expected to double by end of 2014 • Commercial plans with ACOs • Aetna, Blue Cross Blue Shield, Cigna and Anthem/Wellpoint EXPECTED TO GROW
Remember • What is an ACO • Joint accountability • measured quality improvements • cost reduction • patient-centric coordinated services • Across continuum of care • Financial incentives • ACA and ACO • Organizations and Standards • Benefits • Barriers • Future Trends