Download
1 / 13
130 likes | 248 Views
Using CQUINS to improve COPD care on discharge from Acute Trust. Dr Vince Mak Consultant Physician – North West London Hospitals Clinical Lead in Respiratory Medicines Management – NHS London. What is CQUINS?. Commissioning for Quality and Innovation payment framework since 2008

E N D
Using CQUINS to improve COPD care on discharge from Acute Trust Dr Vince Mak Consultant Physician – North West London Hospitals Clinical Lead in Respiratory Medicines Management – NHS London
What is CQUINS? • Commissioning for Quality and Innovation payment framework since 2008 • A form of QoF for Providers – except payment is of money that the Provider has already earned • Provider has to prove it has reached a level of quality before payment made
Monetary Value of CQUINS • 2011/12 –worth 1.5% of total Provider yearly outturn (Up 0.5%) • For NWLH = 1.5% of £250million = £3.75million • 0.3% is allocated to the 2 National CQUINS leaving 1.2% for locally negotiated goals
National CQUINS • 2 Obligatory National CQUINS • VTE Assessment • Improving Patient Experience • VTE target is set at 90% of all eligible patients • Patient experience goal is locally negotiated
Local (Regional) CQUINS • Explicit requirement on commissioners to collaborate in order to agree a single CQUIN scheme per provider • Each scheme has to have the National plus any number of locally agreed CQUINS from a local “Pick List” determined by SHA
What is a Local CQUIN? • CQUIN Goals should be agreed between commissioners and providers, with clinical engagement locally, and should reflect both local priorities and priority areas • Each CQUIN goal must be measurable, using a defined indicator • The number of goals and indicators included within a CQUIN scheme should be determined locally to ensure that improvement is focused appropriately and that the scheme is not unnecessarily complex
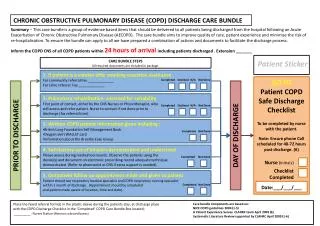
COPD Discharge Bundle • Produced by CHLARC NW London • Care Bundle applied to all patients admitted with known COPD as a primary diagnosis • 5 evidenced based interventions that known to improve quality of care and reduce readmissions and further exacerbations
What is CLAHRC? • CLAHRC NW London (Collaboration in Leadership and Applied Health Research and Care • Alliance of academic and healthcare organisations working to develop and promote a more efficient, accelerated and sustainable uptake of clinically innovative and cost-effective research interventions into patient care • Part of National Institute of Health Research
5 Key Elements of COPD Discharge Bundle • Smoking Cessation • Assessment for Pulmonary Rehabilitation • Disease Education and formulating self management plan with prescribed rescue pack • Check of adequate inhaler technique by competent trainer • Adequate Follow up arrangements made (either community, Hospital OPA or GP)
Discharge bundle as a CQUIN • On NHS London Pick List (of 10) • Taken up by at least 4 Acute Trusts within London so far • Target is 75% of all COPD admissions in first year will have bundle completed by discharge • 90% in second year
Monetary Value of COPD CQUIN • In NWLH Trust – 1.2% of outturn = £3million (0.3% allocated to National CQUINS) • 3-4 local CQUINS chosen (including falls assessment, patients assessed within 12 hours of admission) • Value = £0.75-1million per CQUIN
Outcome • Acute Trusts motivated to perform (£1 million!!!!!) • Patients get ideal care, improved QoL and reduced readmissions • Should significantly reduce expenditure for COPD • Good example of QIPP