Download
1 / 28
560 likes | 3.3k Views
Blood Gases, pH and Buffer system. Part 1. Introduction. An important aspect of clinical chemistry is information on a patient's acid-base balance and blood gas homeostasis. These data often are used to assess patients in life-threatening situations. This lecture discusses:

E N D
Introduction • An important aspect of clinical chemistry is information on a patient's acid-base balance and blood gas homeostasis. • These data often are used to assess patients in life-threatening situations. • This lecture discusses: • the body's mechanisms to maintain acid-base balance and • exchange of gases, carbon dioxide and oxygen, M. Zaharna Clin. Chem. 2009
Definitions: Acid, Base, Buffer • Acid: • asubstance that yields H ions in H2O. • Base: • asubstance that yields a hydroxyl ion (OH). • Buffer: • the combination of a weak acid and its salt, is a system that resists changes in pH. M. Zaharna Clin. Chem. 2009
Acid, Base, Buffer • The relative strengths of acids and bases, their ability to dissociate in water, are described by their dissociation constant (ionization constant - K value) • pK: defined as the negative log of the ionization constant; • that is pH where the protonated and unprotonated forms are present in equal concentration. M. Zaharna Clin. Chem. 2009
Strong acids vs. Strong Base • Strong acids: • have pK value of less than 3.0 • Strong base: • have a pK value greater than 9.0 M. Zaharna Clin. Chem. 2009
Acid-Base balance Maintenance of hydrogen ions: • Body produces 40-80 mmol of H/day, • normal concentration of H in ECF ranges from 36-44 nmol (pH, 7.34-7.44) • Any deviation from the values the body will try to compensate. • >44 nmol/L: altered consciousness, coma- death • <36 nmol/L: neuromuscular irritability, tetany, loss of consciousness- death. M. Zaharna Clin. Chem. 2009
Acid-Base balance • Because pH is the negative log of the cH+ • Decrease in H ion Increase pH • Increase H ions Decrease pH • Arterial blood pH is controlled by: • Buffers • Respiratory System • and Kidneys M. Zaharna Clin. Chem. 2009
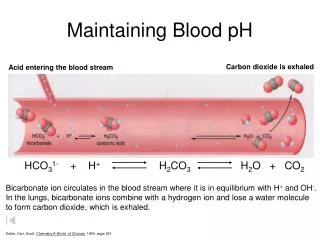
Buffer System: Regulation of H+ • First line of defense to changes in H+ consist of: • weak acid (H2CO3)& its salt (HCO3-) • Add acid to H2CO3& HCO3- system: • the HCO3- combines with H from the acid to form H2CO3. • Add a base to the system: • H2CO3 combines with OH to form H2O and HCO3 • Keeps the body at the correct pH (7.35-7.45) M. Zaharna Clin. Chem. 2009
Buffer System: Regulation of H+ • Bicarbonate – carbonic acid system has low buffering capacity but still an important buffer system for 3 reasons: • H2CO3 dissociates into CO2 & H2O allowing H+ to be eliminated as CO2 by lungs • Changes in CO2 modify the ventilation rate • HCO3- conc. can be altered by the kidneys M. Zaharna Clin. Chem. 2009
Other systems HPO4–2 H2PO4– system Proteins are capable of binding H+ Hemoglobin M. Zaharna Clin. Chem. 2009
Regulation of Acid-Base Balance: Lungs and Kidneys • The lungs and kidneys play important roles in regulating blood pH. • The lungs regulate pH through retention or elimination of CO2 • by changing the rate and volume of ventilation. • The kidneys regulate pH by: • excreting acid, primarily in the ammonium ion, • and by reclaiming HCO3- from the glomerular filtrate. M. Zaharna Clin. Chem. 2009
Regulation of Acid-Base Balance by Lungs • End product of aerobic metabolic process is CO2 • diffuses out the tissue into plasma and RBC • In Plasma & RBCs: • a small amount of CO2 is dissolved • or combined with proteins to form carbamino compounds. • Most of the CO2 combines with H2O to form H2CO3, which quickly dissociates into H+ and HCO3- M. Zaharna Clin. Chem. 2009
Regulation of Acid-Base Balance by Lungs • The dissociation of H2CO3 causes the HCO3- concentration to increase in the RBCs and diffuse into the plasma. • To maintain electroneutrality chloride diffuses into the cell (chloride shift) M. Zaharna Clin. Chem. 2009
Regulation of Acid-Base Balance by Lungs • In the lungs: • The process is reversed. • Inspired O2 diffuses from the alveoli into the blood and is bound to hemoglobin, forming oxyhemoglobin (O2Hb). • The H+ that was carried on the (reduced) hemoglobin in the venous blood is released to recombine with HCO3- to form H2CO3, • which dissociates into H2O and CO2. M. Zaharna Clin. Chem. 2009
Regulation of Acid-Base Balance by Lungs The CO2 diffuses into the alveoli and is eliminated through ventilation. The net effect of the interaction of these two buffering systems is a minimal change in H+ concentration between the venous and arterial circulation. M. Zaharna Clin. Chem. 2009
Interrelationship of the bicarbonate and hemoglobin buffering systems M. Zaharna Clin. Chem. 2009
Regulation of Acid-Base Balance by Lungs • When the lungs do not remove CO2 at the rate of its production (hypovent.) it accumulates in the blood, • causing an increase in H+ concentration. • If, however, CO2 removal is faster than production (hypervent,) • the H+ concentration will be decreased. • Consequently, ventilation affects the pH of the blood. M. Zaharna Clin. Chem. 2009
Regulation of Acid-Base Balance by Lungs • A change in the H+ concentration of blood that results from nonrespiratory disturbances causes the respiratory center to respond • altering the rate of ventilation in an effort to restore the blood pH to normal. • The lungs, by responding within seconds, together with the buffer systems, provide the first line of defense to changes in acid-base status. M. Zaharna Clin. Chem. 2009
Kidney system • Main role is reabsorption of bicarbonate • Kidneys respond to increase or decrease in hydrogen ions by selectively excreting or reabsorbing: • Hydrogen ions • Sodium • Chloride • Phosphate • Ammonia • Bicarbonate M. Zaharna Clin. Chem. 2009
Re absorption of Bicarbonate Reabsorption of bicarbonate (HCO3 –) takes place in the renal tubule cells. Na + is exchanged for H+ ion. H+ ion combines with the HCO3 – and carbonic acid dissociates into H2O and CO2. CO2 diffuses into the tubule cells combining with H2O forming H2CO3. Reabsorption of bicarbonate in the blood system. Urinary H+ combines with HPO4– and NH3. M. Zaharna Clin. Chem. 2009
carbonic anhydrase M. Zaharna Clin. Chem. 2009
Acid-Base Disorders Acidosis (decrease pH) → acidemia Alkalosis (increased pH) → alkalemia metabolic or respiratory A disorder caused by ventilatory dysfunction is termed primary respiratory acidosis or alkalosis. A disorder resulting from a change in the bicarbonate level is termed a nonrespiratory disorder. M. Zaharna Clin. Chem. 2009
Acid-Base Disorders • Body's cellular and metabolic activities are pH dependent • The body tries to restore acid-base homeostasis whenever an imbalance occurs. • This action is termed compensation • Done by altering the factor not primarily affected by the pathologic process. • eg., if the imbalance is of nonrespiratory origin, the body compensates by altering ventilation. • For disturbances of the respiratory component, the kidneys compensate by selectively excreting or reabsorbing anions and cations. M. Zaharna Clin. Chem. 2009
Acid-Base Disorders • Lungs can compensate immediately but: • the response is short term • and often incomplete. • The kidneys compensate are slower to respond (2-4 days) but: • the response is long term • and potentially complete M. Zaharna Clin. Chem. 2009
Metabolic (non-respiratory)Acidosis • Decrease pH, increase H • Bicarbonate decreased (<24 mmol/L) • Caused by: • acid producing substance or process • or reduce excretion of acids • Compensation: • 1o - Respiratory compensation: • Hyperventilation, decrease CO2 in circulation. • 2o -Renal compensation: • increase H ion loss by increasing PO4 and NH4 excretion and retain HCO3 M. Zaharna Clin. Chem. 2009
Respiratory Acidosis • Caused by hypoventilation • decrease the elimination of CO2 in the lungs, it builds up in the blood • decrease in pH, increase in H and HCO3 • Diseases: emphysema, drugs , congestive heart failure, bronchopneumonia. • Compensation • Renal compensation • increase H excretion& increase reabsorption of HCO3- M. Zaharna Clin. Chem. 2009
Metabolic (non-respiratory ) alkalosis • HCO3- increased, H decreased, pH increased • Causes of nonrespiratory alkalosis: • excess administration of NaHCO3 • ingestion of HCO3– producing salts such as Na-lactate, citrate or acetate • excessive loss of acid through vomiting • Compensation • Respiratory compensation • Hypoventilation with CO2 retention • Renal compensation • excrete HCO3 and retain H ions. M. Zaharna Clin. Chem. 2009
Respiratory alkalosis • Decreased CO2, decreased H,increased pH • Causes of respiratory alkalosis include: • hypoxemia; • chemical stimulation of the respiratory center by drugs, such as salicylates; • pulmonary fibrosis. • Compensation • Renal compensation • decrease renal excretion of H ions, HCO3 excreted. M. Zaharna Clin. Chem. 2009