Download
1 / 28
280 likes | 590 Views
Renal function- basic data for students and residents. Department of Paediatrics Section for Pediatric Nephrology University Hospital Motol, Prague . Functions of the kidney. regulation e.g. homeostasis, water, acid/base excretion e.g. urea, creatinine endocrine e.g. renin,

E N D
Renal function- basic datafor students and residents Department of Paediatrics Section for Pediatric Nephrology University Hospital Motol, Prague
Functionsof the kidney regulation e.g. homeostasis, water, acid/base excretion e.g. urea, creatinine endocrine e.g. renin, erythropoietin, 1,25 dihydroxycholecalciferol- conversion only in kidney!
Renal function tests • detect renal damage • monitor functional damage • help determine etiology
glomerular filtration rate (GFR) plasma creatinine plasma urea urine volume urine urea minerals in urine urine protein urine glucose hematuria osmolality Laboratory tests of renal function
Kidney Function • A plumbers view
Kidney – basic data • Urine excreted daily in adults:cca 1.5L • Kidney only ca 1% of total body weight, despite it • The renal blood flow= 20% of cardiac output • Plasma renal flow= PRF ca 600 mL/Min./1.73 M2 • Reflects two processes • Ultrafiltration (GFR): 180L/day • Reabsorption: >99% of the amount filtered
How do you know it’s broken? • Decreased urine production • Clinical symptoms • Tests
Where can it break? • Pre-renal • Renal (intrarenal) • Post-renal (obstruction)
Causes of kidney functional disorders • Pre-renal e.g. decreased intravascular volum • Renal e.g. acute tubular necrosis • Postrenal e.g. ureteral obstruction
glomerular filtration rate=GFR plasma creatinine= Pcr plasma urea-Purea urine volume= V urine urea- Uurea cystatin C in plasma? urine protein urine glucose hematuria osmolality Tests of renal function
Renal Function Tests- Urine volumes • Adults: • 1.5 L/24 htypical in health, • oliguria < 400 mL, • anuria < 100 mL, • polyuria > 3000 mL • Children: ca 1.5 ml/Kg of b.w./1 hour!
Some substances when filtered enter the tubules are not reabsorbed and so 100% excreted= GFR (inulin= gold standard for GFR, creatinine (but this one partially reabsorbed, particularly in uremia, then clearance<GFR Some substances are filtered, enter tubules, and more of the substance is secreted enters the tubules by excretion. Clearance>GFR Some substances are filtered, enter tubules, but are completely reabsorbed, so they did not reach the final urine (e.g. cystatin C) Principle of of Clearance
Glomerular filtration rate • Glomerular filtration= major physiologic responsibility of kidney, GFR used as index of overall excretory function • Methods: • clearence of inulin, creatinine, EDTA and DTPA (=both derivates of acetic acid), cystatin C • GFR= Ux x V(V=volum of urine/ 1 minute or 1 second) • P xx= clearence of substance used
Glomerular filtration rate • Also service of nuclear medicine dptm. • Follow up the inulin clearence, EDTA or DTPA clearence labelling the substances with chromium or Tcm99 Where will you catch the activity with detectors? Never in the kidney or bladder area!!
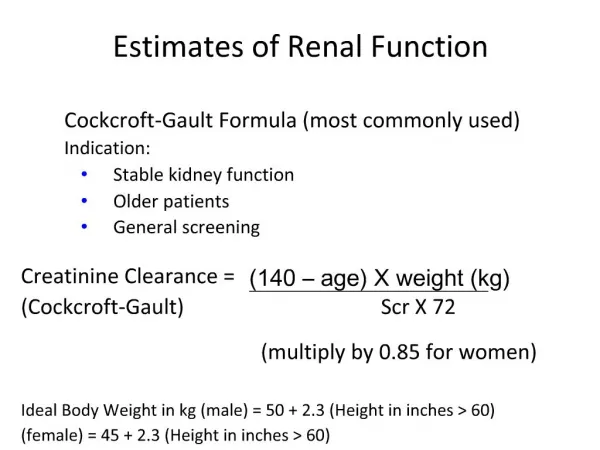
Glomerular filtration rate • GFR in children, value always adapted to the BSA!! Ideal BSA in adults is 1.73m2 • Schwartz equation : GFR= v x 0.808 • Pcr (umol/L) • How to assess easy if plasma creatinine is OK? • Pcr max= Vcm x 0.61 (v= body height in cm
Creatinine and Urea Plasma Concentration- hyperbolic correlation Tendency in individual patients is more important than the one value, ever test if the hydration is OK. In patients with CRI always note also the BSA! Lower limit today not 80 ml/Min. /1.73 m2 but 90 ml/Min./1.73 m2 pCr, pUrea Normal range-> 140 mL/min (100%) 0mL/min (0%) GFR 50%
Plasma urea (BUN) • = BUN (blood urea nitrogen) • Urea: product of protein catabolism • Synthesized by liver, majority excreted by kidney, partially reabsorbed in tubuli • Plasma concentration increases with decreased GFR
Urea cycle aspartate CO2 NH3 Urea Cycle 3 ATP Urea
Enzymatic conductivity rate method for measuring urea Urea + 3H2O urease Urease solution HCO3¯ + 2NH4 + OH¯
Urea in patients with kidney diseases • Useful test but must be interpreted with great care, urea plasma level is more than creatinine dependent on protein intake Most useful when considered along with creatinine • High in high protein intake, low in severe liver dysfunction • Urea EF may be useful in pts. on diuretics
Plasma creatinine and renal functions • Creatine: main storage compound of high energy phosphate needed for muscle metabolism. • Creatinine: anhydride of creatine! Creatine Creatinine (Waste product) H2O
Plasma creatinine vs. GFRnot linear, hyperbolic correlation! [pCreat] Change within an individual patient is usually more important than the absolute value 140 mL/min (100%) 0 mL/min (0%) GFR
Jaffe´ reaction for measuring creatinine, simple, but better is enzymatic method Creatinine + alkaline picrate solution Bright orange/red colored complex absorbs light at 485nm (many interfering substances in blood Can be minimized using rate method)
Analytical methods (Cr) • Normal range Pcr Male 0.6-1.2 mg/dL, Female 0.5-1.0 mg/dL Be careful in children!! Remember themax. plasma creatinine value!!
BUN: creatinine ratio • Pre-renal disorders • BUN:Cr ratio >20 • Renal disorders • BUN:Cr nl but both elevated • Post-renal
Osmolality of urine • Measures urine concentrating ability • Depends on # of particles, not size or charge • Largely due to ADH (anti-diuretic hormone) • Can reach maximum of 1200 mOsm/L • Normal range: 300-900mOsm/L, plasma 285+10 • prior to collection, fluid intake restricted, first void submitted for evaluation • Measuring using the fact of freezing point depression
Standardized renal concentration capacity test • 1. Voiding completely at 9 p.m. (WC) • 2. Desmopressin administration (since 2006 as nasal spray). DDAVP is a Czech invention !! • 3. Collection of urine (9 p.m. – 7 a.m.) • 4. Testing of urine osmolality in this sample (not the morning urine only!) • 5. The lower limit of normal value= 950 mOsm/kg of urine • 6. Short testing- Desmopressin, collection for 4 hours only= at least 900 mOsm/kg of urine
Urine dipsticks • Strip impregnated with reagents for the substances in question within a urine sample • Substance level can be altered in the setting of pathology within the urinary tract • Measured substances: • Modern dipsticks with multiplied zones: • Protein, hemoglobin, glucose, urobilinogen, nitrite, leukocytes, specific gravity, and pH • Should be a tool everywhere on the level of primary care!!!