Download
1 / 61
610 likes | 748 Views
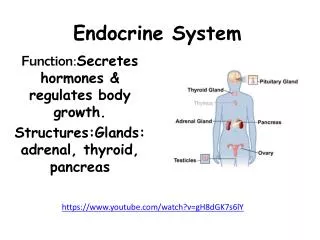
ENDOCRINE SYSTEM. THYROID GLAND. Thyroid hormones affect nearly all body tissues Dysfunctions cause profound effects Three hormones: T 3 ; T 4 ; calcitonin Thyroid hormone’s main component is iodine

E N D
THYROID GLAND • Thyroid hormones affect nearly all body tissues • Dysfunctions cause profound effects • Three hormones: • T3 ; T4 ; calcitonin • Thyroid hormone’s main component is iodine • Minimum daily requirement of I= 80 mcg; more like 500mcg (contained in bread, water, and iodized salt)
THYROID • Thyroid gland can store large quantities for months • S/S may not appear for months • Works on negative feedback system; TRH signals TSH which stimulates thyroid gland • Most hormone is bound to protein
THYROID • Functions: • Metabolism: increase rate, accelerate food utilization for energy, excites mental processes • Growth: in children accelerates growth • Carbohydrate: stimulates metabolism, including insulin secretion • Fat: enhances fat metabolism • Body wt: production relates inversely to body wt (does not stimulate appetite) • CV: causes vasodilation, increased cardiac output and heart rate, increased systolic B/P by 10-20 mm but diastolic may drop the same • Respiration: increases O2 use, rate, and depth • GI: increases appetitie, absorption,motility • CNS: speeds mental processes
THYROID • Assessments: • Swallowing • Skin changes • Tolerance to heat or cold • Weight changes • Palpitations • Drugs • Radiation to neck or surgery • Head trauma • Alcohol • Growth rate • Appetite • Menstrual periods • BEGIN WITH INSPECTION, LOOKING FOR LUMPS, PUFFINESS, FACIAL EXPRESSIONS, ENLARGED TONGUE, VOICE, HAIR, VISION, NAILS, AND MUSCLE ACHES.
THYROID • Diagnostic tests: • Thyroid panel: T3 & T4; free and bound; • RAIU: radioactive iodine uptake; uses radioactive iodine and scan thyroid as it uses iodine. Given PO, IV, or liquid; only use small amt. no risk, do before scan with contrast • Stimulation tests • Scans • Ultasound • Biopsy
THYROID • Hyperthyroidism: • Involves excessive hormone production • Leads to hypermetabolism • Signs and symptoms: thyrotoxicosis • Stimulates heart, protein synthesis, breakdown>buildup leading to negative nitrogen balance (degradation); hyperglycemia; increased fat metabolism • Caused by two etiologies: • Increased iodine uptake (Grave’s, goiter, adenoma • Low iodine uptake (subacute and silent)
THYROID • Grave’s disease: toxic diffuse goiter • Most common • Strikes women, 20-30. • Multisystem syndrome, affecting eyes, skin, bones • Increased thyroid hormone as well as goiter • No sure cause: autoimmune disorder • Generally emotional upset precedes symptoms • Has heredity component
THYROID • Assessment: • Increase appetite but slight wt loss • Dyspnea • Decreased heat tolerance • Menstruation may decrease or stop • Increased bowel movements or diarrhea • Nervous, irritable, restless • Speak rapidly; laugh inappropriately • Exopthalamus (BUG-EYE) • Moist skin, thinning hair, elbows red; clubbing of nails (Plummer’s nails), hyperpigmentation (vitiligo- milk-white patches) • Tremors, weakness • Tachycardia, atrial fibrillation; widened pulse pressure • Fine, soft hair; moist skin • Hyperactive deep tendon reflexes
THYROID • Diagnostic tests: • Elevated T3, T4 • RAIU • No response to TRH • Below normal TSH • Thyroid scan
THYROID • Interventions: • Record vital signs • Rest, frequent linen changes, cool environment • Drugs to reduce hormone: can cause thyroidstorm • PTU • Tapezole • Iodine-radioactive; cells are destroyed • Lithium • Inderal: not used on clients with asthma or heart disease • Watch for agranulocytosis: fever, sore throat, rash • Treatment does not correct infiltrative opthalopathy; use tears, elevate head, diuretics for edema; prednisone
THYROID • Surgical intervention: • May perform total or subtotal • Treat with drugs to return to near normal thyroid function prior to surgery • Give Lugol’s solution or SSKI (saturated solution of potassium iodide) prior to OR to firm thyroid, reduce vascularity which can reduce bleeding • Give in milk, OJ, sip thru straw so as not to discolor teeth • Watch for toxicity: buccal mucosal swelling, excessive salivation, skin reactions • May receive Inderal to reduce cardiac problems • Teach T,C, & DB; support head, explain about risk for hoarseness and soreness
THYROID • After surgical assess: • Vital signs • Voice-may be hoarse; usually temporary • Neuromuscular functioning • Expect moderate drainage; check back of neck • Respiratory distress- use humidified air • Laryngeal stridor, paralysis, tetany • Keep in semi-Fowler’s • Avoid strain on suture line- avoid neck extension • Keep emergency drugs: • O2, suction, trach tray, calcium gluconate • Monitor for transient hypothyroidism, damage to voice, nerves, hypocalcemia, and tetany
THYROID • Thyroid storm: • Crisis situation- usually caused by Grave’s • Life-threatening • Uncontrolled hyperthyroidism • Develops quickly and triggered by stress; over-palpation of gland • Fever, tachycardia, systolic hypertension, GI, restlessness, confused, psychotic • Even with treatment, 25% mortality rate
THYROID • Hypothyroidism: • Deficiency in thyroid hormone • Leads to low metabolism with build-up of metabolites • Metabolites with water accumulate within cells, cause edema, called myxedema • Myxedema coma: rare but can occur; heart becomes flabby, chambers increase in size, CO decreases; life threatening; high mortality rate
THYROID • 3 TYPES: • HYPOTHYROIDISM: adult onset; tissue destruction is most probable cause • CRETINISM: • Profound hypothyroidism in infants • All developmental aspects are retarded • Severe brain damage can occur • If caught early, can prevent retardation • JUVENILE HYPOTHYROIDISM: • Begins during childhood, Hashimoto’s disease, caused by drugs, autoimmune • Affects growth and sexual maturation
THYROID • Assessments: • Changed sleeping habits (increased) • Lethargy, • HA, wt gain • Cold intolerance • Dyspnea • Constipation • Menorrhagia • Muscle aches • Anorexia • Lack of expression • Cool, dry, skin, yellow tint, rough, thick, scaly • Dry hair, coarse, lusterless • Enlarged tongue • Speech slow and deliberate with hoarse voice • Impotence and infertility • Decreased blood pressure; bradycardia; dysrhythmias; decreased urinary output
THYROID • Diagnostic tests: • Below-normal T3 & T4 • Above-normal TSH • Above-normal TRF • Above-normal creatinine phosphokinase • Anemia
THYROID • Interventions: • Requires life-long replacement hormone • Synthetic usually used T4 (Levothyroid, Synthroid, Noroxine) • Start with lowest dose possible and work way up every 1-3 weeks • With known cardiac problems, always use lowest dose possible • T3 (Cytomel) has more rapid effect. • Euthroid (Liotrix)– combined T3 & T4 • Make sure client knows to continue with meds even if he feels better • Avoid sedation if possible
THYROIDITIS • Inflammation of thyroid • Three types: • Acute: bacterial; pain, malaise, fever, dysphagia; treat with antibiotics • Subacute: viral infection; fever, chills, dysphagia, pain, hard & enlarged gland; treat symptoms; antivirals • Chronic: (Hashimoto’s)- auto immune, invade thyroid with antibodies and lymphocytes causing tissue destruction; treat with thyroid hormone • Administer thyroid hormones; surgery; promote comfort and teaching
THYROID CANCER • 4 types • Surgery is treatment- total • Suppressive doses of thyroid for 3 months after surgery • Ablation- laser destruction of tissue • chemotherapy
PARATHYROIDS • Parathyroid hormone corrects calcium deficiency by promoting calcium conservation by kidneys, stimulating calcium release by bone, enhance calcium absorption from GI, & reduce serum phosphate levels. • Works on negative feedback control • In kidneys, causes calcium to be reabsorbed with release of phosphorus • Stimulates kidneys to convert Vit D to a metabolite that allows for PTH to work on bone • In bone, helps convert osteoblasts to osteoclasts, promoting bone breakdown and release of calcium. • Acts on GI to stimulate absorption of calcium (must have calcitriol). • Calcitonin from thyroid causes inhibition of Ca++ release from bones
PARATHYROID • Hyperparathyroidism: • Primary: • Faulty PTH regulation; adenoma, genetics, CA, radiation, hyperplasia; occurs more commonly in women, 35-65 • Secondary: • Compensatory response to defective homeostasis, chronic renal failure, malabsorption disorders • Tertiary: • Compensates for secondary malfunction to primary, leading to overgrowth of gland and overproduction and secretion
PARATHYROID • All three lead to increased calcium and decreased phosphorus
PARATHYROID • Assessments: • Urine calcium increase and kidneys fail to concentrate urine • Phosphorus excretion increases • Enhances sodium, potassium, amino acids, bicarbonate (acidosis leading to excretion of Ca++ • Polyuria • Renal calculi • Bone demineralization (breakdown): • Bone pain • Pathologic fractures • Cystic bone disease
PARATHYROID • Other assessments: • Weakness, wt. loss, fatigue • HA, depression • Renal colic pain, back pain, • Hematuria, renal calculi, cholelithiasis • Anorexia, vomiting, constipation • Peptic ulcer (stimulates gastric HCL) • Increase heart contractility; decreased automaticity • Increased sensitivity to digitalis • Hypertension • Depressed reflexes- hyporeflexia • Confusion, irritability, mood swings
PARATHYROID • Diagnostic tests: • Serum PTH: elevated • Calcium: elevated (>10.5mg/dl; 5.2mEq/L • Kidney stones • Phosphorus: decreased • X-rays; CT; MRI: look at bone density and demineralization • PTH infusion test: (Ellsworth-Howard excretion test); give IV PTH, hourly urine samples looking for phosphorus • Calcitonin stimulation test: if cancer suspected; use calcium gluconate
PARATHYROID • Interventions: • Surgery (usually remove only three) • Stabilize calcium levels prior to surgery • Hemorrhage • Laryngeal paralysis • Difficulty swallowing • Respiratory distress • Transient hypoparathyroidism • Tetany • Muscle cramps • Hyperactive tendon reflexes • Prolonged QT on EKG • Positive Chvostek’s and Trousseau’s signs
PARATHYROID • Interventions: • Medical treatment: • Rehydration with isotonic fluids • Diuresis • Mobilization • Restrict intake of calcium (thyazides and Vit D. • Monitor EKG • Drugs: • Phosphates: Neutra-phos • Calcitonin: IV; IM- decrease release from skeletal areas; increased excretion by kidneys • Calcium chelators ( bind calcium) Plicamycin: mithramycin; cytotoxic agents; watch for thrombocytopenia • Steroids: inhibit Vit D • Estrogen • Alpha & beta blockers • cimetidine
PARATHYROID • Hypoparathyroidism • Too little PTH leading to decreased calcium and increase phosphorus • 3 types • Iatrogenic: • Most common, resulting from surgery of neck removing glands, radiation, or other trauma • Idiopathic: • Early onset and late onset; autoimmune; genetic causes of absent glands, pernicious anemia, ovarian failure • Functional: • Long term hypomagnesemia causes this (alcohol, malabsorption)
PARATHYROID • Assessments: • Neuromuscular problems, increased excitability, tetany, muscle cramps, tingling, numbness, hyperreflexia • Tetany leads to anxiety; leads to hyperventilation; leads to hypocapnia and alkalosis, which worsens hypocalcemia • Seizures, laryngeal spasms • Personality changes • Increased ICP • Nausea, vomiting • Dysrhythmias, decreased contractility, reduced CO • Cataracts, dry skin, scaly, coarse • Alopecia • Bands or pits on teeth
PARATHYROID • Diagnostic tests: • Serum calcium: low • Serum phosphorus: high • Serum magnesium: normal to low • Serum PTH: low • Urinary creatinine: low • Urinary excretion of calcium: high • X-ray; MRI; CAT scans
PARATHYROID • Interventions: • Treatment focuses on preventing tetany and correcting hypocalcemia • IV calcium gluconate or calcium gluconate • Do not use saline, promotes calcium and sodium excretion • Avoid bicarbonate, cause precipitation • Vit D and calcium supplements • Ergocalciferol (Vit D2 ); Rocaltrol; may use combined therapy of oral and IV initially • Need 1 gram of calcium daily if using Vit D • Life-long therapy • Emergency airway if laryngeal spasms occur • Foods high in calcium but low in phosphorus- milk, yogurt, processed cheese.
ADRENAL GLANDS • Widespread effects, confusing clinical picture • S/S mimic many other disorders • Survival depends upon prompt diagnosis and treatment
ADRENAL GLANDS • Cortex secretes glucocorticoids and mineralocorticoids • ACTH from anterior pituitary is controlled by CRF • Other factors controlling release include stress, circadian rhythms • ACTH peaks at 6am, Cortisol at 8am; lowest level at midnight • With decreasing cortisol, ACTH is stimulated and released • Stress prompts release of glucocorticoids to promote metabolism of proteins, amino acids, fatty acids, and glucose
ADRENAL GLANDS • Mineralocorticoids, aldosterone, is controlled by renin-agiontension system • Renin is increased by blood volume, blood pressure, and Na+ • Renin lead to angiotension II production and aldosterone formation • K+ & Na+ directly affect aldosterone release • Increased K+ increases aldosterone and Na+ decreases aldosterone • Epinephrine and norephinephrine are produced, but because brain produces we can survive without adrenal medulla
ADRENAL GLAND • Assessments: • Most disorders have slow, gradual onset and progression • Changes early are subtle, hard to detect • Weight changes • Fatigue • Apathy • Depressed or neurotic • Worsens with increased stress • Physical appearance may be a clue
ADRENAL GLAND • Physical assessment: • Responds appropriately, but facial expressions do not match • Normal weight • Increased secondary sex characteristics • Fat distribution abnormal • Poor skin turgor • Purplish striae on abdomen • Pitting edema • Hyperpigmentation • Hair distribution is abnormal • Muscle weakness
ADRENAL GLANDS • Diagnostic tests: • Secreted in minute amounts, therefore most sensitive tests are RAI • Remember: if anxious, will affect results of some tests • Samples must be timed!!
ADRENAL GLANDS • Cushing’s syndrome: hypercortisolism • Cortisol excess • Affects more women than men • Primary: • Usually a neoplasm • Secondary: • Pituitary or hypothalamus disorder causing increased ACTH; adrenal hyperplasia • Iatrogenic: • Excessive use of steroids (prednisone) • Artifically increases cortisol, suppresses ACTH, causing adrenal atropy • S/S are of hyperfunction
ADRENAL GLAND Cushing’s • Assessments: • Fatigue, muscle wasting • Frequent infections, slow wound healing • Suppressed immune response ( can mask S/S); kill lymphocytes • Truncal obesity, buffalo hump, moon-shaped face, scrawny arms and legs (PICKLE WITH LEGS) • Fragile skin, purplish striae on abdomen, buttocks, breasts, bruises • Masculinization in women, hirsutism (increased hair growth), acne • Hypertension • Osteoporosis • Labile emotions • Abnormal sleep patterns • Nitrogen, carbohydrate, and mineral metabolism • Elevated blood glucose
ADRENAL GLANDS CUSHING’S • Diagnostic tests: • Cortisol: high with no circadian variation • Urinary levels of steroid metabolites: high • RBC and granulocytes: high • X-rays, MRI, CAT scans • Dexamethasone suppression test: give 1 mg at night, test at 8am; high level
ADRENAL GLAND CUSHING’S • Interventions: • Treat underlying cause; stop steroids • Remove tumors of pituitary or adrenalectomy ( uni or bi lateral) • Drugs: • Mitotane to inhibit cortisol synthesis ( watch for adrenal crisis!! • Cyproheptadine: ACTH inhibitor • Aldactone: mineralocorticoid antagonist to relieve hypertension and hypokalemia
ADRENAL GLAND CUSHING’S • Complications: • Fluid and e-lyte imbalances • Hypertension: Na+ and water retention • CHF: excess volume in compromised heart • Hypokalemia • Ventricular dysrhythmias: due to CHF and hypokalemia • Increased risk for infections & fractures • Skin breakdown
ADRENAL GLAND INSUFFICIENCY: ADDISON’S • Suppressed adrenocortical function and hormones • May precipitate “adrenal crisis”: life-threatening • Primary: • Addison’s- rare, chronic disorder • 90% gland usually destroyed before symptoms appear • Secondary: • Reduced ACTH secretion caused by pituitary disease or exogenous steroid administration; more common • Impairs stress response by reducing cortisol, aldosterone, and androgens
ADRENAL GLAND ADDISON’S • Assessments: • Muscle weakness and fatigue (especially during stress) • Nausea, vomiting, diarrhea, abdominal pain • Salt craving • Anxiety, restlessness, irritability, and confusion • Orthostatic hypotension • HYPOGLYCEMIA & HYPERKALEMIA • Hyperpigmentation (ONLY PRIMARY DISEASE HAS THIS) • Knees, elbows, nipples, palm creases, scars( bronzed, “dirty tan”) • Small black freckles on neck, face; bluish splotches on mucous membranes
ADRENAL GLANDS ADDISON’S • Diagnostic tests: • Serum cortisol: low • Urinary metabolites: low • ACTH: • ACTH stimulation: elevated cortisol=Addision’s; low cortisol=secondary disease • Hyperkalemia • Hyponatremia • Hpochloremia • Fasting hypoglycemia • BUN elevated; hematocrit HCT elevated
ADRENAL GLANDS ADDISON’S • Interventions: • Lifelong therapy with replacement • Drugs: • Cortisone: twice daily, increase dose for stressful times • Florinef: aldosterone replacement • Salt food liberally • Avoid fasting • Eat high carbs and proteins • Always wear medic alert identification • Carry emergency kit with 100mg hydrocortisone for injection • Prevent acute exacerbations • Avoid salt and fluid restriction with diuretics; may lead to crisis
ADRENAL GLANDS • Complications: • Adrenal crisis: due to insufficiency; can occur gradually or abruptly (acute adrenal insufficiency) • Potentially lethal • Occurs in individuals who don’t respond to therapy; increased stress without increased meds; abrupt corticosteroid withdrawal • ALWAYS WITHDRAW STEROIDS THERAPY GRADUALLY
ADRENAL GLANDS ADRENAL CRISIS • Treatment: • Restore volume with D5NS • Be sure to assess fluid status frequently • Cortisol q 6 hr. (Solu-Cortef IV): if given with saline, proves adequate to replace Aldosterone • Do not give methyleprednisolone (Solu-Medrol: lack mineralocorticoid effects) • Reduce anxiety