Download
1 / 22
240 likes | 413 Views
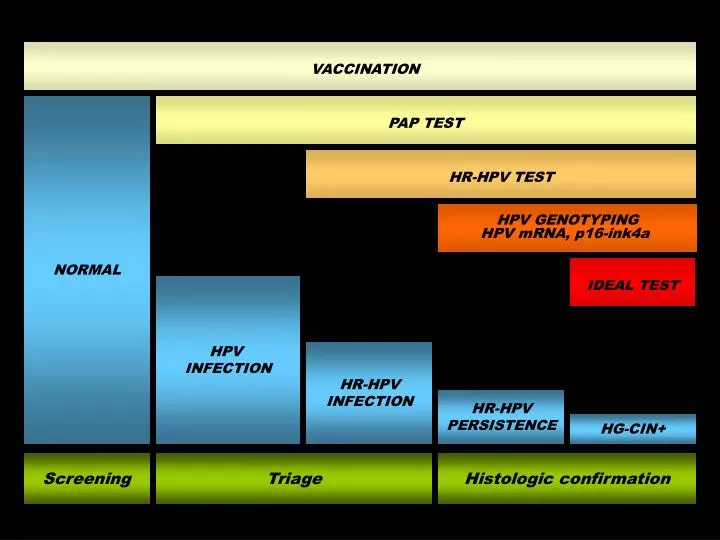
VACCINATION. NORMAL. PAP TEST. HR-HPV TEST. HPV GENOTYPING HPV mRNA, p16-ink4a. HPV INFECTION. IDEAL TEST. HR-HPV INFECTION. HR-HPV PERSISTENCE. HG-CIN+. Screening. Triage. Histologic confirmation. Technologies for the detection of HPV DNA.

E N D
VACCINATION NORMAL PAP TEST HR-HPV TEST HPV GENOTYPING HPV mRNA, p16-ink4a HPV INFECTION IDEAL TEST HR-HPV INFECTION HR-HPV PERSISTENCE HG-CIN+ Screening Triage Histologic confirmation
Technologies for the detection of HPV DNA • Ideally, a HPV test should allow the detection of multiple, clinically relevant HR-HPV types, identify individual types, provide quantitative informations about viral load of each individual type, be easy to perform, reproducible, highly specific and sensitive, rapid, automatable and of low cost. • The ideal HPV test does not exist yet • A limited number of tests is available that perform differently and have a specific clinical applications • Translation of HPV testing into clinical practice requires setting rigorous standars of test performance and characteristics • Basically, HPV tests can be divided into: • Tests for HPV DNA detection and typing • Hybrid Capture 2 (HC2) • PCR-based assays • HPV-based biomarkers
Established HPV test technologies and their performances* * Modified from Iftner & Villa, JNCI Monographs, 2003
The different performances of HPV tests impact on the estimated prevalences of infections and the clinical significance of HPV status Analytical sensitivity should be clearly differentiated from clinical sensitivity when assessing the clinical relevance of a HPV test Snijders PJF et al. J Pathol, 2003
PROs and CONs of available HPV technologies • Choice of a test format involves a tradeoff between performance (accuracy, reproducibility and coverage), cost, laboratory requirements, ease of integration in current protocols of screening and diagnosis • HC2 is available in large scale format, does not require specific laboratory facilities, does not depend on PCR amplification, provides a semiquantitative estimate of viral load, has been largely validated for screening • HC2 does not allow identification of individual types and have some degree of cross-reaction between types • PCR-based assays allow individual HPV type identification and are more analytically sensitive than HC2. • PCR-based assay vary in sensitivity, specificity and coverage depending mainly on the type of primers and the lenght of amplicons; in general, they show good agreement but their performance in detecting distinctive types especially in multiple infections can be different.
Full spectrum genotyping • Detection of individual types in multiple infection • Distinction of incident from prevalent HPV infections • Post-vaccination surveillance • Monitoring of HPV type burden in different populations or settings • Prediction of type-specific oncogenic risk and/or persistence • Triage of HPV-positive women with negative or low-grade cytology or follow-up of women with previous SIL • Persistence of any HPV type for 1 yr or more increases the RR of CIN3+ 42.9 times (Koshiol J et al , Am J Epidemiol 2008) • Cytologicaly negative women testing positive for HPV16/18 are at higher risk for prevalent and incident CIN3+ than HPV16/18-positive women with L-SIL (Castle PE et al. JNCI 2005) • Baseline positivity for HPV16/18 is associate with 4-6x risk of CIN3+ at 10 years compared to other HPV types (Khan MJ et al, JNCI 2005) • Women with abnormal cytology and multiple HPV infections are at greater risk for CIN2+ (Dal Bello B et al. J Med Virol in press)
The number of HPV types is correlated with CIN severity * Spearman Rho = 0.094, p = 0.001 ** Sperman Rho = 0.67, p <.001
The number of HPV types is correlated with CIN severity Odds ratios and 95% confidence intervals (CI) of histological outcomes according to number of infecting HPV types, age and previous SIL/CIN Negative Reference CIN1 0 HPV Reference 1 HPV 50,78 24,0 – 107,49 2 HPV 107,66 50,13 – 231,22 ≥ 3 HPV 177,02 61,48 – 510,0 <.001 Age 0,95 0,94 – 0,97 Previous SIL/CIN 0,43 0,19 – 0,94 CIN≥2 - 0 HPV Reference carcinoma 1 HPV 38.4 1,.5 – 101,4 2 HPV 121,4 46,3 – 318,4 ≥ 3 HPV 817 251 – 2655 <.001 Age 0,97 0,95 – 0,99 Previous SIL/CIN 0,46 0,20 – 1,07
Current vaccines target less than 50% of CIN2+ associated HPVs The effect of the number of infecting HPV types on the risk of CIN is independent of the main oncogenic types targeted by current vaccines Variables All w/o HPV-16 w/o HPV-6,11, 16, 18 Negative Reference Reference Reference CIN1 Single infection Reference Reference Reference Multiple infection 11.5* (7.5-17.5) 16.15* (9.6-27.0) 14.40*(7.4-27.9) Age 0.95* (0.94-0.97) 0.96* (0.94-0.97) 0.96* (0.93-0.98) Previous SIL/CIN 0.34* (0.15-0.77) 0.62 (0.22-1.79) 1.01 (0.35-2.90) CIN≥2/ Single infection Reference Reference Reference carcinoma Multiple infection 27.6* (17.2-44.2) 19.28*(10.9-34.1) 21.53*(10.5-43.9) Age 0.97** (0.95-0.99) 0.99 (0.97-1.01) 1.00 (0.98-1.03) Previous SIL/CIN 0.36** (0.15-0.82) 1.79 (0.67-4.76) 1.36 (0.43-4.27) * p<0.005, ** p0.05 Assuming that the observed distribution of viral types is representative of the general population, current vaccines would prevent an expected fraction of any CIN and of CIN≥2, of 30% and 43%, respectively
Guidelines for HPV testing requirements in primary screening* • Most candidate HPV DNA assay differ in clnical specificity due to differences in the detection rates of transient infections with low viral loads • At present, only HC2 and GP5+ /6+ -PCR-EIA have been consistenly validated in large prospective cohorts or RCTs. • Clinical sensitivity for CIN2+ not less than 90% of HC2 in women 30 years • Clinical specificity for CIN2+ not less than 98% of HC2 in women 30 years • Interlaboratory agreement not less than 87% • Specific infrastructure for nucleic acid amplification • Laboratory accreditation for clnical molecular testing • Monitoring of laboratory performances by proficiency testing • Standardization requirements extend largely beyond • the perfomances of the specific assay * Meijer C et al, Int J Cancer 2009, 124:516-520
Quality control and standardization requirement for HPV testing* Specimen collection Specimen transport medium DNA extraction method STANDARDIZED PROTOCOLS AND REAGENTS ONGOING QUALITY CONTROL PCR primers and amplification Type-specific probes Interpretation of data * Modified from Gravitt PE et al. Vaccine 2008, 26S:K42-K52
The enormous advancement in knowledge on the biology of SIL can be translated into new screening strategies and pathologic criteria • HPV-related biomarkers • HPV E6-E7 mRNA (NASBA) • HPV viral load • HPV integration • p16-ink4a IHC • Methylation profiles • TERC-gain • Telomerase/topoisomerase IIa • Proliferation /cell cycle markers • Quiagen’s fast HPV technology • E6 strip test
Clinical applications of HPV DNA testing • Triage of undetermined cytology • Test-of-cure after excision of HG-CIN • Triage of L-SIL • Primary screening • Post-vaccination surveillance • Detection of persistent infections • Inter-individual transmission • Epidemiological surveillance
HPV testing for the triage of ASCUS • A cytological diagnosis of ASCUS underlays CIN2 in 8,7% [6.9-10.5] of cases and CIN3 in 3.9% [2.4-5.5], on average 43% of women are HPV+. • Twenty-two studies using HC2 were considered (Vaccine, 2008, 26S, K29-K41). • Pooledsensitivity of HPV DNA detection in predicting CIN2 and CIN3 is 93.1%[91.1-95.1] and 95.5%[92.7-98.2], respectively. • Pooledspecificity for CIN2 and CIN3 is 62,3%[57.6-67.1] and 60.5%[52.9-68.2], respectively. • Repeat Pap smear was taken in 7 studies, HC2 sensitivity was on average 14% higher for the detection of CIN2+ considering a cytological cut-off of ASCUS (ratio 1.14 [1.08-1.20]) with a similar specificity (ratio 0.99 [0.88-1.10]). • The ALTS study provides data of 2 year follow-up with serial cytology for an outcome of CIN3 +. Three repeat smears had a sensitivity of 60% for a cytological cut-off of CIN2 with 12% colposcopy and sensitivity of 97% for a cut off of ASCUS with 73% colposcopy. These figures compare with a sensitivity of 92% for HPV test with a 53% colposcopy rate
HPV testing for surveillance after the treatment of HG-CIN • Following excision of HG-CIN, 10% of women may experience a recurrence over a 4 year period. • Risk is recurrence is higher in older women, has increased in recent years and is lifelong (Strander B et al BMJ, 2007). • Sixteen studies were considered that were heterogeneous with respect to design, timing of follow-up, type of HPV DNA assay and inclusion criteria. • Sensitivity of HPV DNA detection in predicting treatment failure ranges from 67% to 100%, pooled 94.4%[90.9-97.9](Vaccine, 2006, 24 suppl, S78-89). • Specificity varied between 44% and 100%, pooled 75%[68.7-81.4]. • Compared with follow-up cytology, HPV testing was more sensitive (ratio 1.16 [1.02-1.33]) with no significant loss of specificity (ratio 0.96 [091-1.0]). • Compared with histological assessment of surgical margins, sensitivity was higher (ratio 1.31 [1.11-1.55]) and equally specific (ratio 1.05 [0.96-1.15]). • Women with HPV16 infections should be monitored more closely (Murat G et al, Gynecol Oncol 2007).
HPV testing for the triage of L-SIL • On average 74.4% of women with L-SIL are HPV+, this limits the capacity of the test to stratify women according to disease severity. • Following a cytological diagnosis of L-SIL, histologically confirmed CIN2 and CIN3 are present in 17.6% [11.8-23.3] and 7.4% [2.9-12.0]. This proportion can be substantially lower for women aged 35 (Ronco G et al, Eur J Cancer 2007; Cuzick J et al., Lancet 2003). • Eleven studies are available for meta-analysis and systematic review. • Pooled sensitivity of HC2 triage for an outcome of CIN2 is 97.2%[95.6-98.8] and 97.1%[94.0-100] for CIN 3 (Vaccine, 2006, 24 suppl, S78-89). • Pooled specificity an outcome of CIN2 is 30.6%[22.7-38.6] and 26.1%[15.1-37.1] for CIN 3. • The value of HPV testing in this setting depends on management strategies of L-SIL (follow-up with repeat smear or immediate colposcopy), and the accuracy of colposcopy/biopsy (false negative colposcopy rates as high as 30% have been reported in histological diagnoses of CIN2+).
HPV testing in primary screening • Pooled data for 25 cross-sectional studies and 3 randomized studies(Vaccine, 2008, 26S, K29-K41). • 5-15% of women undergoing screening are HPV-DNA positive with a inverse correlation with age • Pooled absolute sensitivity of HC2 for CIN2+ is 89.7%[86.4-93.0] with a wide range (50 to 100%) mainly according to geographic areas. • Pooled specificity in excluding CIN2+ is 88.2% [86.2-90.1]. • Sensitivity and specificity of HC2 for CIN+ in studies for Europe and North America is consistently higher, 98.1% [96.8-99.4] and 91.7% [90.3-93.1], respectively, with low values of heterogeneity. • Relative sensitivity was 33% [20-47%] higher than cytology for a cut-off of ASCUS, whereas relative specificity was 6% [2-8%] lower. • Adding cytology to HPV DNA testing adds little or no sensitivity and reduces specificity.
HPV testing in primary screening • When HPV DNA testing is used as part of the initial screening, either alone or in combination with cytology, lower rates of CIN2 are detected at subsequent rounds. • This further increases if HPV-positive women are triaged with cytology • In a recent multinational cohort study, the cumulative proportion of CIN3+ at 6 years for HPV-negative women at baseline was one third that for PAP-negative women (0.27% vs. 0.97%). By comparison, the proportion observed at 3 years for PAP-negative women was 0.51% (Dillner J et al, BMJ 2008). • In the Portland study, the NPV of CIN3+ for double-negatives over a 5 year period was 99.91% [99-85-99.9] corresponding to 9/10.000 women that will develop CIN3+ compared with 30/10.000 cytology-screened women (Sherman ME et al, JNCI 2003). • These arguments support the idea that screening intervals can be safely extended to at least 5 years
HPV testing in primary screening: conclusions • HPV DNA testing is substantially more sensitive than cytology to detect CIN2+, whereas it is less specific primarily due to the detection of transient infections that do not produce cytologic changes. • In this context, basic principles would suggest that the more sensitive test (HPV DNA) is applied first and the more specific (cytology) is used for triage. • Several RTCs and mathemathical models support the cost-efficacy and the increased accuracy of HPV DNA testing as a primary screening modality • Additional advantages of HPV DNA testing compared to cytology: • objective and automable test allowing better quality control and reducing medico-legal litigation • cytology can be reserved for triage of a minority of samples allowing the widspread introduction of more accurate test and better quality controls and trained cytologists • reduces the need for triage of ASCUS/L-SIL • allows longer screning intervals and possibly later onset of screen • allows monitoring of vaccinated women
Future scenario of primary cervical screening Women aged 25-64 yrs HPV DNA TESTING HPV-negative HPV-positive NORMAL 5-YEAR RECALL CYTOLOGY Normal/bordeline L-SIL+ HPV TEST & CITOLOGY at 6-12 months COLPOSCOPY HPV & cytology negative L-SIL+ NORMAL 5-YEAR RECALL COLPOSCOPY HPV-positive and/or borderline cytology HPV TEST & CITOLOGY at 6-12 months Cuzick J et al. Vaccine, 2008, 26S, K29-K41).
HPV testing in primary screening: open questions • Should be introduced within organized programs rather than used in an opportunistic setting • Organized screening should consider separate protocols according to age and vaccination status • CIN2 remains an equivocal clinical endpoint • The optimal management for HPV-positive cytology-negative women should be defined • The role of multiple HPV infections and persistence should be clarified • Further biomarkers for truly progressive epithelial lesions are needed for triage of low-grade abnormalities • The impact of vaccination on HPV type circulation and performance of HPV DNA testing and cytology requires attention • Ultimately, clinical evidences should be translated into new health policies