Download
1 / 31
310 likes | 321 Views
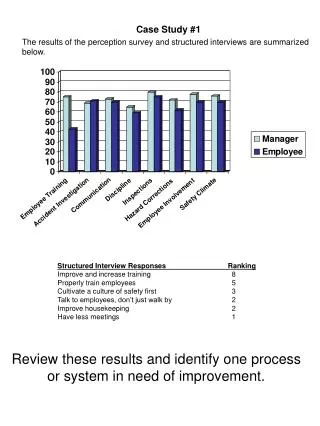
Case Study 1. Harry Kellermier, M.D. Question 1. This is a 70 year-old male who presented with paresthesias and clumsiness in his right upper extremity. What are the abnormal findings seen in these radiographs?. Answer. Mass lesion In the left frontoparietal region Irregular

E N D
Case Study 1 Harry Kellermier, M.D.
Question 1 This is a 70 year-old male who presented with paresthesias and clumsiness in his right upper extremity. What are the abnormal findings seen in these radiographs?
Answer • Mass lesion • In the left frontoparietal region • Irregular • Peripherally enhancing • Surrounding edema
Question 2 What is your differential from these radiographs?
Answer Malignant glioma; Metastasis; Lymphoma; Abscess; Subacute infarct.
Question 3 EXAMINE SMEAR. An intraoperative consultation was requested. Describe the microscopic findings on this slide. Click here to view slide
Answer • Reactive astrocytes with abundant eosinophilic cytoplasm • Background acute and chronic inflammatory cells • Macrophages • Vessels with plump, reactive endothelium
Question 4 What would the intraoperative consultation be based on the previous smear? (A: Category such as Defer, Reactive, or Neoplastic; B: More specific diagnosis)
Answer • Defer • Reactive and inflammatory changes
Question 5 EXAMINE H&E. The permanent section from the intraoperative specimen has returned from histology. Describe the microscopic findings on this slide. Click here to view slide.
Answer • Fibrovascular tissue • Necrotic tissue • Inflammatory infiltrate consisting of acute and chronic inflammatory cells • Macrophages
Question 6 What additional studies would you like based on this permanent specimen.
Answer • GMS • Gram stain • Check microbiology results
Question 7 EXAMINE GRAM STAIN: What do you see on this slide? Click here to view slide.
Answer Slender, branching gram positive rods
Question 8 EXAMINE GROCOTT STAIN. What do you see on this slide? Click here to view slide.
Answer Filamentous, branching rods
Question 9 What organisms are in your differential?
Answer • Nocardia • Actinomyces • Streptomyces
Question 10 What additional stain would you order (pictured below)? • Ziehl-Nielsen • Fite • Luxol Fast Blue • Warthin-Starry • Modified Gram Stain
Answer The answer is B. Fite.
Question 11 By what route of infection did this patient acquire Nocardia?
Answer Nocardia species are widely distributed in the environment. The usual route of infection is by inhalation and pulmonary involvement, with subsequent spread to other sites. Nocardia asteroides complex accounts for approximately 80% of cases of noncutaneous invasive disease. According to some reports, the CNS is the second most commonly affected organ with some studies citing secondary CNS involvement in approximately 25% of cases. Despite this apparent affinity for the CNS, Nocardia accounts for only approximately 2% of all brain abscesses. Patients who develop nocardial brain abscesses are typically immunosuppressed. Commonly affected groups include organ transplant recipients, persons with connective tissue diseases, HIV, pulmonary diseases and underlying malignancies. Less commonly, Nocardia may present as a meningitis, diffuse cerebral infiltration, or granulomas.
Epidemiology • 0.3-1.3 per 100,000 people per year • Higher in immunocompromised patients • Causative organisms • Streptococcus species- 34% • Viridans 13%, pneumoniae 2% • Staphylococcus species- 18% • Aureus 13%, epidermidis 3% • Gram negative enteric- 15% • Proteus 7% • Klebsiella, E.Coli, enterobacteriae all 2% • Nocardia- 1%
Predisposing conditions • Otitis/mastoiditis- 32% • Sinusitis- 10% • Hematogenous- 13% • Meningitis- 6% • Postoperative- 9% • Unknown- 19%
Location • 81% of the time only a single lesion was identified • Frontal lobe- 31% • Temporal lobe- 27% • Parietal lobe- 20% • Cerebellar and brainstem- 13%
Diagnosis and outcome • Aspiration with culture and smear! • MRI>CT scan • DWI hyperintense signal with correlating hypointense signal on ADC had a 96% sensitivity and specificity for differentiating abscess from other intracranial cystic mass • Outcome • 20% Mortality • 57% Good outcome
References • Brouwer et al. ‘Clinical characteristics and outcome of brain abscess: Systemic review and meta-analysis.’ Neurology, 1/29/2014