Download
1 / 27
290 likes | 523 Views
California Trauma System Summit - 2008. Trauma Systems Development: An ACS Perspective. Robert C. Mackersie, M.D., FACS Professor of Surgery, UCSF Director, Trauma Services, SFGH Past Chair, ACS-COT Trauma Systems Planning & Evaluation. 523,780 patients 18 states J.Trauma 2004.

E N D
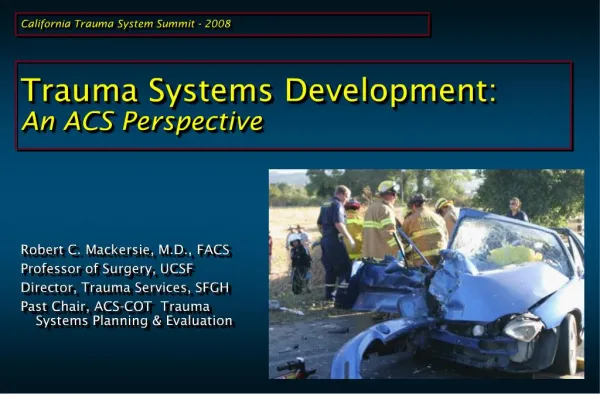
California Trauma System Summit - 2008 Trauma Systems Development: An ACS Perspective Robert C. Mackersie, M.D., FACS Professor of Surgery, UCSF Director, Trauma Services, SFGH Past Chair, ACS-COT Trauma Systems Planning & Evaluation
523,780 patients 18 states J.Trauma 2004
360,743 patients - California JACS 2003
facs.org American College of Surgeons COMMITTEE ON TRAUMA Consultation Program for Trauma Systems American College of Surgeons
American College of Surgeons COMMITTEE ON TRAUMA Consultation Program for Trauma Systems American College of Surgeons
1992 MTCSP: What a system IS. • Leadership • System Development • Legislation • Finances • Injury Prevention & Control • Human Resources • workforce / education • Prehospital • EMS, transport, communication, disaster • Definitive Care • TCs, transfers, rehab • Information systems • Evaluation • Research
2006 Model Trauma System Planning and Evaluation:What a system DOES. • Assessment • systems needs vrs. resources • injury epidemiology • ‘burden of injury’ & system performance • cost effectiveness • Policy Development • Comprehensive authority • Trauma Plan & modifications • Prevention public policy • Establishes evidence-based system guidelines • Is driven by assessment • Assurance • Use of laws, regulations, standards • System PI & oversight body • Integration of primary, secondary, tertiary prevention • Strategic planning (workforce, all-hazards preparedness, etc)
American College of Surgeons COMMITTEE ON TRAUMA Consultation Program for Trauma Systems
ACS-COT Trauma Systems Evaluation • Consultative, not verification (no one fails!) • Multi-disciplinary structure • Independently derived recommendations (ACS integrity) • Politically ‘inert’ • Consensus-based process • Basis = Inclusive trauma system (MTCSP) • Basis = best interests of the patient • Collaborative development: • (HRSA, NHTSA, CDC, NASEMSD, ACEP) • based on national objectives (HRSA, NHTSA)
Trauma Systems: Common Problems • Reluctance to use enabling legislation • Inconsistent or non-integrated leadership • Unauthorized leadership • Absent or ineffective state (STACs) or regional advisory committees (RTCC) • Trends towards exclusive systems • no resources, commitment, interest • lack of consistent specialty availability • over-triage, over-transfer to designated centers
Trauma Systems: Common Problems • Lack of funding: system & under-compensated care • No comprehensive trauma plan • Limited (or non-existent) system-based PI • Limited regional organization & participation by NTC facilities • Ends of the spectrum poorly integrated (silo’ing) : prevention & rehabilitation in particular
Trauma Systems: Common Problems • Structure does not allow strong medical direction for state/regional trauma sys • Incomplete, inadequate MOU between sending & receiving hospitals • Limited, often inadequate public and legislative education RE trauma system importance & needs • various others…
Access: Obstacles in trauma system participation • Physician staff commitment • Lifestyle: long, irregular hours, sleep deprivation • Practice: opportunity costs, restriction, reimbursement, malpractice • Intimidating, verification / designation requirements • Lack of knowledge / experience • Financial risk: • Under-funded care, contractual agreements • Limited transfer $$: DSH, local tax subsidies • On-call fees for physicians • Lack of specific state/regional funding
California trauma “system” • Serving disaster-prone, dispersed population • Provides coverage for very urban & very rural regions • County –based & de-centralized • Optional – but embraced by most counties • Relies on local versus regional/State-wide oversight • State & many local systems under-funded • State/regional structures insufficiently authorized • Comprehensive, state-wide plan pending • Wide variations in county trauma system configurations & practices (“inconsistencies” • State-wide trauma registry pending
System development • Educate & build legislative & public support • Establish enabling legislation • Fund the system exclusive from TCs • Needs assessment (link to prevention) • Write comprehensive trauma plan • Adopt operational standards & verification • Develop oversight structures • Initiate system PI plan & oversight • System development driven by PI / CQI • Perform external consultative review
“Get a plan” (G. Cooper, ~2004) • System structure: • lead agency, STAC, RTCCs, role of TCs & community • System leadership positions within structure (TMD, TPM) • Regional structure: ‘X’ regions? (not 32 or 58) • System-wide needs assessment • Injury epidemiology in the State • Type, number, location of TCs & flow patterns • Human resource pipeline • System oversight responsibilities & PI plan • Disaster preparedness (current surge cap=~14%)\ • Establish process/program for injury surveillance
Funding the system • SYSTEM = STATE, REGIONAL, COUNTY • Motor vehicle fees, fines, penalties (non-MV also) • 911 system surcharges • Intoxication / DUI offense fees • Controlled substance act or weapons violation fees • “Play or pay” fees for non-participating hospitals • Tobacco & ETOH taxes • Property tax supplements • Tribal gaming • Hospital licensure linked to participation in TS • Use of destination / activation fees
Oversight committees • Use experience of States with well established state-wide trauma systems & organizations • Expand the STAC • Develop & fund positions for system oversight / admin. • State Trauma Medical Director + State Program staff (SB261) • Regional program staff + admin staff (Romero SB261) • Recruit system leadership (medicine, government, business, law) • Using the TP, establish & authorize advisory cmtes • Define role of RTCC relative to LEMSAs (“integrated”) • Develop system PI program tailored to regions
Other key elements • Acute care access: assess adequacy of existing TCs – level & location • Assess adequacy of existing resources, county-by-county • Cultivate participation in state/regional trauma system • institutional & provider incentives • Accessible, state-wide registry
System-based (versus center-based) PI • Old model designed for developing systems • Relies more on shared center-derived PI issues (MAC model) • Focus on provider vrs. system errors • Limited use of system indicators • Limited focus on PI process effectiveness
System-wide PI will drive development • system preventable deaths • access to trauma system • time to definitive care • triage errors • failed / delayed transfers • provider errors (TAC/MAC) • access to rehab • prevention deficiencies • benchmarking for TCs
RTCC tasks • Adopt standards, analyze performance • Develop P&Ps • transfers, re-triage, • Create ‘operational’ MOUs between centers • Educational ‘give-backs’ • PI driven outreach • Link to state registry & prevention activities • ID & monitor outcome measures & benchmarks