Download
1 / 20
210 likes | 516 Views
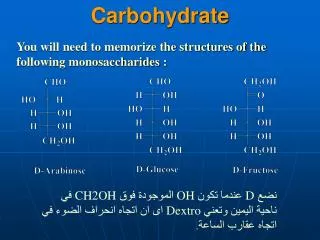
CARBOHYDRATE TOLERANCE. Glucose tolerance is the ability to regulate the blood glucose concentration after the administration of a test dose of glucose (normally 1 g/kg body weight) Diabetes Mellitus decrease glucose tolerance.

E N D
CARBOHYDRATE TOLERANCE Glucose tolerance is the ability to regulate the blood glucose concentration after the administration of a test dose of glucose (normally 1 g/kg body weight) Diabetes Mellitus decrease glucose tolerance. Normal blood glucose levels are 50-100 mg per desi liter (500/180 - 1000/180 mmol / l). Depend on the intake of food before the test. Patients do not febrile, not in stress.
500 8 Glucose 400 6 300 4 200 2 Insulin 100 0 0 noon 8 am 6 pm midnight 8 am Blood glucose levels are relatively constant Plasma glucose (mmol/l) Plasma insulin (pmol/l) meals Time of day
There is also an opinion that under the normal curve160 mg/100 ml one hour and120 mg/100 ml two hours after administration of glucose.
BLOOD GLUCOSE LEVELS Sources:1) Food2) Gluconeogenesis3) Glycogenolysis Maintenance of blood glucose by the liver with glycogenolysis and gluconeogenesis, is under hormonal control (glucagon or if blood glucose drops very promptly epinephrine)
Coordination between organs is needed to control blood glucose levels Glycogen Food consumption Gluconeogenesis Glucose muscle adipocytes liver
55% Oxidation 45% Brain 75% Glycogenolysis 10% Muscle Glucose 20% Glycolysis (muscle) 25% Gluconeogenesis 25% Re-uptake (liver, gut) 60% from lactate Carbohydrate metabolism Glucose turnover (basal state)
If blood glucose ↓ pancreatic glucagon released, glucagon activates adenylyl cyclase, an enzyme catalyzes formation of cAMP from ATP, cAMP activates the cAMP-dependent protein kinase, which in turn will converts phosphorylase kinase b to phosphorylase kinase a (ATP as phosphate donors). Active phosphorylase kinase catalyzes phosphorylase b to phosphorylase a. Phosphorylase a break down glycogen and generate G 1P. With glucantransferase and debranching enzyme glycogenolysis will proceed until the liver depleted with glycogen. G-1P converted to G-6P and G-6Pase splits the phosphate. Glucose then enters the circulation.
Glycogenn Glycogenn -1 + G-1P G-6P G ( in the Liver )
Other hormones (in addition to glucagon and epinephrine)affecting blood glucose levels:InsulinGHACTHCortisolThyroid
INSULIN • Secreted in inactive formProinsulin C peptide + insulin C peptide is more easily measuredSubstances or chemicals which stimulates insulin secretion:glucose, amino acids, free fatty acids, ketone bodies, glucagon, tolbutamide and secretine.In contrast epinephrine inhibits Insulin secretion • Insulin entrance of G into cells except liver, erythrocytes and neuronal cells.
Insulin MW 5808 PC2 (PC3) PC3 Proinsulin C peptide Ca2+-dependent endopeptidases A Chain B Chain
Growth Hormone: Growth hormone may affect levels blood glucose by activating Hormone Sensitive Lipase. The resulting fatty acids, and derivatives (acetyl-CoA and ketone compounds) causes inhibition of glucose consumption by peripheral tissues
ACTH (Adreno Cortico Tropic Hormone) • Affect the metabolism of carbohydrates together with GH increase gluconeogenesis Cortisol: enhance gluconeogenesis
Renal function in Carbohydrate Metabolism • As a “safety clap“. If blood glucose ↑ , some will be excreted through the kidneys (renal threshold)Renal threshold: 170 - 180 mg / dl.Glucosuria occurredTubule reabsorption capability350 mg / min.
55% Oxidation 45% Brain 75% Glycogenolysis 10% Muscle → Glucose 20% Glycolysis (muscle) 25% Gluconeogenesis 25% Re-uptake (liver, gut) 60% from lactate Carbohydrate metabolism Glucose turnover (basal state)
Biomedical importance • Normal metabolism: hunger if not prolonged, sports, pregnancy and lactation • Abnormal metabolism: lack of certain foodstuffs, as well as enzyme deficiencies or because of abnormal hormone secretion. The most interesting disease to study is diabetes mellitus ( DM ).
Glycolysis: Pyruvate kinase enzyme hemolytic anemia.Malignant tumor ↑ lactic acidHeart can not tolerance unaerobic glycolysis Oxidation of pyruvic acid: vitamin deficiency vit. B1 beri-beri Glycogen: abnormal accumulation of I VIII MP Shunt: G6PD deficiency hemolytic Fructose: Essential Fructosuria, "hereditary" fructose intoleranceSorbitol: ↑ peristalsis Diabetes Mellitus: ↓ glucose utilization
Hemolytic can be caused by deficiency of thefollowing enzymes:PFK-1 (phosphofructo kinase-1)Pyruvate kinaseG6PD (glucose 6 phosphate dehydrogenase) High dietary fructose or fructose infusioncan cause:↓ inorganic phosphate (Pi) ↓ ATP synthesisDecreases in inhibition of Purine synthesisby ATP ↑ Uric acid (uric acid)