Download
1 / 24
240 likes | 349 Views
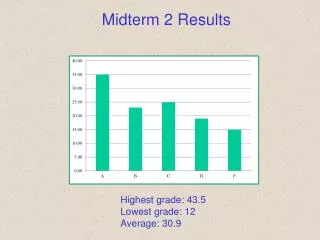
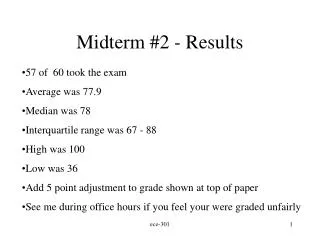
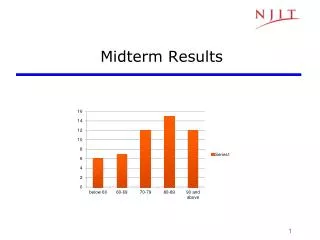
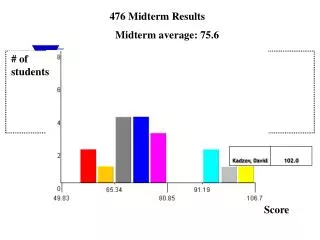
Midterm results - Grades B to A+, mostly low A. Significance of FDA approval Need it to sell device, drug If FDA approved device harms you, can you sue for medical damages? Riegel vs Medtronic says no Why? Supreme court interprets law intended to

E N D
Significance of FDA approval Need it to sell device, drug If FDA approved device harms you, can you sue for medical damages? Riegelvs Medtronic says no Why? Supreme court interprets law intended to prevent States from adding to regulatory requirements as preventing tort suits under state law – see article by Jostin So do you want FDA review to be rigorous?
If FDA approves a device (or drug) for 1 indication, can it be used for another indication? Yes – “off label” use Could you sue if damaged by an off-label use?
Dhruva et al reviewed Summary of Safety and Effectiveness Data reports from all FDA PMAs for cardiovascular devices 2000-7 Issues – Are study endpoints well defined? Are FDA guidelines met? Are the guidelines fair? Drug evaluations often have control groups, double-blind designs, large # pts. Device trials often have smaller # pts., use historical controls – is this too lax?
Pretend you are on review committee for cryoablation catheter
Cardiac Cryoablation Catheter and Console System 2.0 INDICATIONS FOR USE cryoablation of the conducting tissues of the heart in the treatment of patients with atrioventricular nodal reentrant tachycardia (AVNRT). Why is there data for AVT, AF as well as AVNRT if the indication is only AVNRT?
5.0 DEVICE DESCRIPTION … • 8.0 POTENTIAL ADVERSE EFFECTS OF THE DEVICE • * cardiac arrest and/or death; • *cardiac perforation • *catheter entrapment in cardiac structures • requiring surgical intervention; • * coronary artery spasm/dissection/thrombosis • * gas embolism with possible tissue infarction; • *heart block, partial or complete • * hemorrhage; • * hemothorax; • *myocardial infarction • Is this a class I, II or III device?
9.0 SUMMARY OF PRECLINICAL STUDIES… 9.4 ANIMAL TESTING performed in over 275 dogs… 10.0 SUMMARY OF CLINICAL STUDIES The study was designed as a nonrandomized, single-arm, multicenter study to assess the safety and effectiveness of the device used percutaneously in the treatment of AVNRT, AVRT and refractory AF in subjects acting as their own controls. Could it have been randomized?
Endpoints for the study were: • *procedural safety - absence of serious complications • *acute procedural success - non-inducibility of • sustained SVT at the end of the procedure. • chronic success - no recurrence of sustained SVT • at 3-6 mo. follow-up • objective performance criterion (OPC) as described in the • FDA guidance, "Cardiac Ablation Catheters Arrhythmia • Indications for Use; Guidance for Industry
Table 1. Endpoint Criteria from FDA Guidance Endpoint Tgt Value 95 % Confid. Bound Acute Success > 95 % >85 % Chronic Success > 90 % >80 % Major Complications < 2.5 % < 7 % Should these be used, as they are from Guidance document for RF ablation catheters?
Demographic Data of Enrolled Subjects (n=166) Diagnosis n age AVNRT 103 50± 15 AVRT 51 39± 13 AF 12 73±11 AF, atrial fibrillation; AVRT, atrioventricular reentrant tachycardia;
Safety Evaluation Subjects with Adverse Events (n=166) AVNRT AVRT AF All n 103 51 12 166 # (%) with acute major complication 3 (3) 4 (8) 0 (0) 7 (4.2) Eight (8) acute major complications were reported in 7/166 patients (4.2%, upper bound 8.5%). The clinical study safety results exceeded the safety objective performance criteria of 2% with an upper bound of 7.5% Is this enough to disqualify?
Effectiveness Evaluation %, (lower bound CI %) Diagnosis N Acute Success Chronic Success AVNRT 103 91 (82) 93 (85) AVRT 49 69 (51) 88 (69) AF 12 67 (29) 75 (28) Overall 164 83 (76) 91 (85) Guideline >95 (>85) >90 (>80) Cryomapping effect was demonstrated in 64% (87/135) of subjects attempted. One AVNRT subject had a cryomnapping related adverse event (transient AV block lasting 25 seconds).
Your recommendation? Panel voted to approve, subject to submission of a post-approval study to evaluate the rate of AV block. The indication of cryomapping not be approved. CDRH DECISION CDRH determined that the OPCs should not be used to evaluate the safety and effectiveness of the device in the AVNRT subgroup. As a result, the device system was evaluated on its merits… The sponsor demon- strated reasonable assurance of safety and effectiveness.. The cryomapping feature should be enabled for use … The labeling should include a warning to indicate that the effectiveness of the cryomapping feature has not been established.
Next panel – Avastin (antibody to factor that promotes blood vessel growth in tumor) Genentech, Inc submitted two efficacy supplements to the Biologics License Application (BLA) for Avastin to support label expansion for first-line treatment of metastatic breast cancer in combination with docetaxel …and to support conversion from accelerated approval to regular approval for first-line treatment of metastatic breast cancer.
Avastin in combination with paclitaxel received accelerated approval in 2008 based on the results of a randomized, multicenter, open-labeled trial of avastin with paclitaxel or paclitaxel alone that enrolled patients with HER-2 neu negative breast cancer who received no previous chemotherapy for metastatic disease. The addition of avastin resulted in a 52% increase in progression-free survival (HR 0.48, 95% CI 0.39, 0.61; p< 0.0001) with an observed 5.5-month difference in median PFS, based on an independent radiographic review. There was no significant difference in overall survival. Sounds pretty good, but what is progression-free survival (PFS), why use it rather than survival or disease-free survival as a measure of success?
How did they measure PFS? Might it be subject to subjective judgments? Was the study double-blind? Baseline or PFS-determining radiographic scans were missing in 10% of the patients and 34% of the patients were not followed until an IRRC-determined PFS event or the end of the study. In addition, there was a high rate of discordance (50%) between investigator and independent review determined PFS events. Raw data were mean PFS of 5.8 months in controls vs 11.3 months in avastin group. How this is “52% increase” in PFS I can’t say.
Some committee members raised the concern that, given the uncertainties in the PFS effect size due to missing data, patients could be offered false hope. The initial committee voted 5-4 against approval, but were overridden in view of 5 month PFS increase.
Follow-up studies Trial #1 (AVADO) 736 pts., taxol alone vstaxol + low (or high) dose avastin. Low (high) dose avastin added 0.8 (or 0.9) months to PFS. Is that a long time? Why did 5 months drop to <1 month? Safety data showed an increase in serious adverse events in the avastin groups. Actual survival was higher (but not statistically significantly) in the non-avastin group.
Trial #2 (RIBBON) 1237 pts., drug A (or B) +avastin. With drug A (or B), avastin added 1.2 (or 2.9) months to PFS. Serious side-effects were ~ 2x higher in the avastin groups. Avastin is approved for lung and colon CA Do you vote to approve avastin for metastatic breast CA, or to reverse the FDA’s original approval? Would physicians be able to use avastin for breast CA if FDA withdraws its approval?
Other reasons for controversy – cost $50,000-100,000/year; earns Genentech $3.5B/yr ‘Roy Vagelos, a former chief executive of Merck who is considered an elder statesman of the industry, said in a recent speech that he was troubled by a drug, which he would not name but which was a clear reference to Avastin, that costs $50,000 a year and adds four months of life. “There is a shocking disparity between value and price,” he said, “and it’s not sustainable.”’ http://www.nytimes.com/2008/07/06/health/06avastin.html
What ELSI issues are posed by regulation of expensive drugs with minimal but non-zero benefit, used to treat life-threatening illnesses? What is your view?
Next week – ethical issues in research Famous “unethical” studies in the past Tuskeegee (syphillis), Willowbrook(hepatitis) Were they unethical when proposed? How have standards changed? Could what went wrong be prevented? Do genetic studies today pose similar risks?