Download
1 / 1
10 likes | 123 Views
Long-term Outcomes of an Interdisciplinary Weight Management Clinic for Youth with Special Needs Meredith Dreyer Gillette PhD 1, 2 , Cathleen Odar Stough MA 1 , 3 , Shelly Summar MSEd , RD, LD 2 , Janelle Gerling MOT 2

E N D
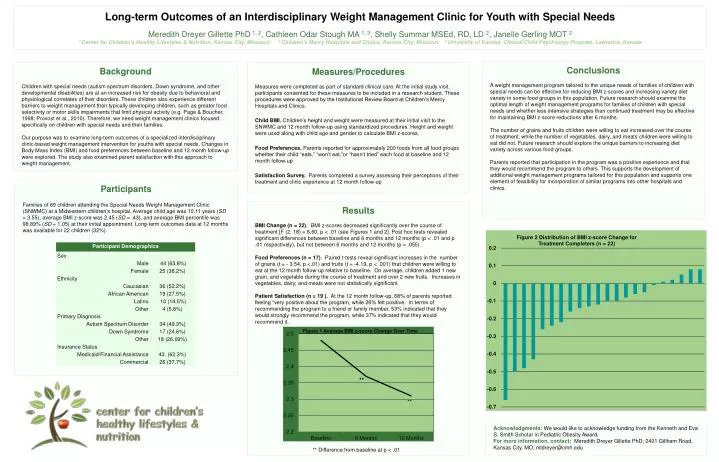
Long-term Outcomes of an Interdisciplinary Weight Management Clinic for Youth with Special Needs Meredith Dreyer Gillette PhD 1, 2, Cathleen Odar Stough MA 1, 3, Shelly SummarMSEd, RD, LD 2, Janelle Gerling MOT 2 1 Center for Children’s Healthy Lifestyles & Nutrition, Kansas City, Missouri; 2 Children’s Mercy Hospitals and Clinics, Kansas City, Missouri; 3 University of Kansas, Clinical Child Psychology Program, Lawrence, Kansas Conclusions A weight management program tailored to the unique needs of families of children with special needs can be effective for reducing BMI z-scores and increasing variety diet variety in some food groups in this population. Future research should examine the optimal length of weight management programs for families of children with special needs and whether less intensive strategies than continued treatment may be effective for maintaining BMI z-score reductions after 6 months. The number of grains and fruits children were willing to eat increased over the course of treatment, while the number of vegetables, dairy, and meats children were willing to eat did not. Future research should explore the unique barriers to increasing diet variety across various food groups. Parents reported that participation in the program was a positive experience and that they would recommend the program to others. This supports the development of additional weight management programs tailored for this population and supports one element of feasibility for incorporation of similar programs into other hospitals and clinics. Background Children with special needs (autism spectrum disorders, Down syndrome, and other developmental disabilities) are at an increased risk for obesity due to behavioral and physiological correlates of their disorders. These children alsoexperience different barriers to weight management than typically developing children, such as greater food selectivity or motor skills impairments that limit physical activity (e.g. Page & Boucher, 1998; Provost et al., 2010). Therefore, we need weight management clinics focused specifically on children with special needs and their families. Our purpose was to examine long-term outcomes of a specialized interdisciplinary clinic-based weight management intervention for youths with special needs. Changes in Body Mass Index (BMI) and food preferences between baseline and 12 month follow-up were explored. The study also examined parent satisfaction with this approach to weight management. Measures/Procedures Measures were completed as part of standard clinical care. At the initial study visit, participants consented for these measures to be included in a research student. These procedures were approved by the Institutional Review Board at Children’s Mercy Hospitals and Clinics. Child BMI. Children’s height and weight were measured at their initial visit to the SNWMC and 12 month follow-up using standardized procedures. Height and weight were used along with child age and gender to calculate BMI z-scores. Food Preferences. Parents reported for approximately 200 foods from all food groups whether their child “eats,” “won’t eat,”or “hasn’t tried” each food at baseline and 12 month follow-up Satisfaction Survey. Parents completed a survey assessing their perceptions of their treatment and clinic experienceat 12 month follow-up Participants Families of 69 children attending the Special Needs Weight Management Clinic (SNWMC) at a Midwestern children’s hospital. Average child age was 10.11 years (SD = 3.55), average BMI z-score was 2.45 (SD = .43), and average BMI percentile was 98.89% (SD = 1.05) at their initial appointment. Long-term outcomes data at 12 months was available for 22 children (32%). Results BMI Change (n = 22). BMI z-scores decreased significantly over the course of treatment [F (2, 18) = 6.60, p < .01 (see Figures 1 and 2]. Post hoc tests revealed significant differences between baseline and 6 months and 12 months (p < .01 and p .01 respectively), but not between 6 months and 12 months(p = .055). Food Preferences (n = 17). Paired t-tests reveal significant increases in the number of grains (t = - 3.54, p <.01) and fruits (t = -4.19, p < .001) that children were willing to eat at the 12 month follow-up relative to baseline. On average, children added 1 new grain, and vegetable during the course of treatment and over 2 new fruits. Increases in vegetables, dairy, and meats were not statistically significant. Patient Satisfaction (n = 19 ). At the 12 month follow-up, 68% of parents reported feeling “very positive about the program, while 26% felt positive. In terms of recommending the program to a friend or family member, 53% indicated that they would strongly recommend the program, while 37% indicated that they would recommend it. ** Acknowledgments: We would like to acknowledge funding from the Kenneth and Eva S. Smith Scholar in Pediatric Obesity Award. For more information, contact: Meredith Dreyer Gillette PhD; 2401 Gillham Road, Kansas City, MO; mldreyer@cmh.edu ** ** Difference from baseline at p < .01Baseline at p < .01