Download
1 / 1
10 likes | 99 Views
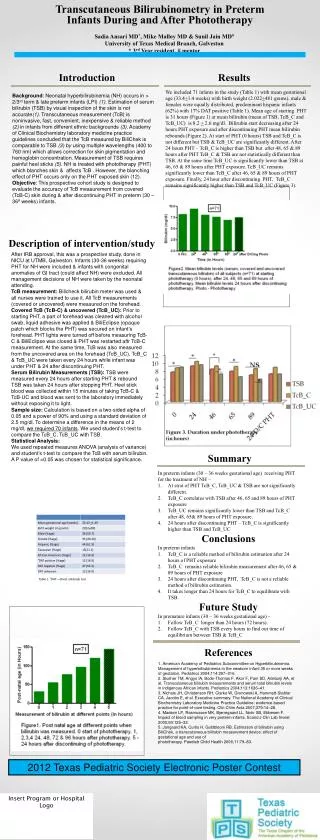
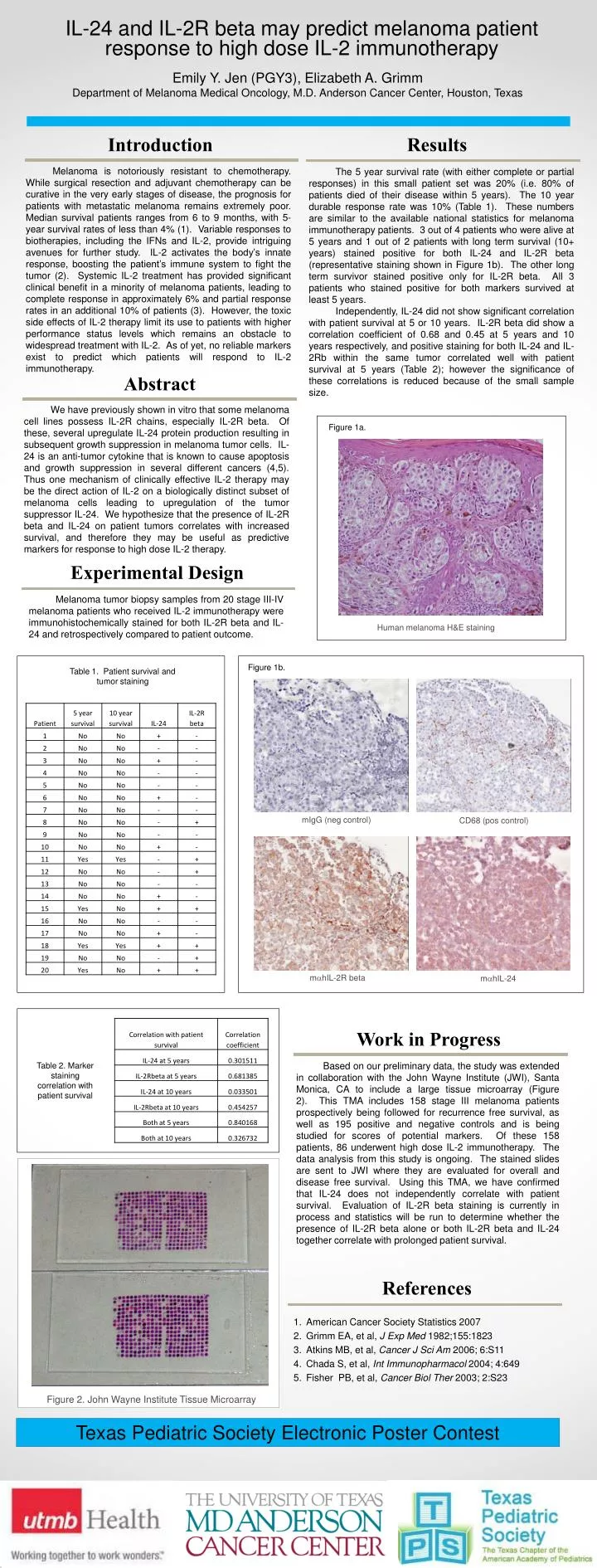
IL-24 and IL-2R beta may predict melanoma patient response to high dose IL-2 immunotherapy. Emily Y. Jen (PGY3), Elizabeth A. Grimm Department of Melanoma Medical Oncology, M.D. Anderson Cancer Center, Houston, Texas. Introduction. Results.

E N D
IL-24 and IL-2R beta may predict melanoma patient response to high dose IL-2 immunotherapy Emily Y. Jen (PGY3), Elizabeth A. Grimm Department of Melanoma Medical Oncology, M.D. Anderson Cancer Center, Houston, Texas Introduction Results Melanoma is notoriously resistant to chemotherapy. While surgical resection and adjuvant chemotherapy can be curative in the very early stages of disease, the prognosis for patients with metastatic melanoma remains extremely poor. Median survival patients ranges from 6 to 9 months, with 5-year survival rates of less than 4% (1). Variable responses to biotherapies, including the IFNs and IL-2, provide intriguing avenues for further study. IL-2 activates the body’s innate response, boosting the patient’s immune system to fight the tumor (2). Systemic IL-2 treatment has provided significant clinical benefit in a minority of melanoma patients, leading to complete response in approximately 6% and partial response rates in an additional 10% of patients (3). However, the toxic side effects of IL-2 therapy limit its use to patients with higher performance status levels which remains an obstacle to widespread treatment with IL-2. As of yet, no reliable markers exist to predict which patients will respond to IL-2 immunotherapy. The 5 year survival rate (with either complete or partial responses) in this small patient set was 20% (i.e. 80% of patients died of their disease within 5 years). The 10 year durable response rate was 10% (Table 1). These numbers are similar to the available national statistics for melanoma immunotherapy patients. 3 out of 4 patients who were alive at 5 years and 1 out of 2 patients with long term survival (10+ years) stained positive for both IL-24 and IL-2R beta (representative staining shown in Figure 1b). The other long term survivor stained positive only for IL-2R beta. All 3 patients who stained positive for both markers survived at least 5 years. Independently, IL-24 did not show significant correlation with patient survival at 5 or 10 years. IL-2R beta did show a correlation coefficient of 0.68 and 0.45 at 5 years and 10 years respectively, and positive staining for both IL-24 and IL-2Rb within the same tumor correlated well with patient survival at 5 years (Table 2); however the significance of these correlations is reduced because of the small sample size. Figure 2. John Wayne Institute Tissue Microarray Abstract We have previously shown in vitro that some melanoma cell lines possess IL-2R chains, especially IL-2R beta. Of these, several upregulate IL-24 protein production resulting in subsequent growth suppression in melanoma tumor cells. IL-24 is an anti-tumor cytokine that is known to cause apoptosis and growth suppression in several different cancers (4,5). Thus one mechanism of clinically effective IL-2 therapy may be the direct action of IL-2 on a biologically distinct subset of melanoma cells leading to upregulation of the tumor suppressor IL-24. We hypothesize that the presence of IL-2R beta and IL-24 on patient tumors correlates with increased survival, and therefore they may be useful as predictive markers for response to high dose IL-2 therapy. Figure 1a. Experimental Design Melanoma tumor biopsy samples from 20 stage III-IV melanoma patients who received IL-2 immunotherapy were immunohistochemically stained for both IL-2R beta and IL-24 and retrospectively compared to patient outcome. Human melanoma H&E staining Figure 1b. Table 1. Patient survival and tumor staining mIgG (neg control) CD68 (pos control) mhIL-2R beta mhIL-24 Work in Progress Table 2. Marker staining correlation with patient survival Based on our preliminary data, the study was extended in collaboration with the John Wayne Institute (JWI), Santa Monica, CA to include a large tissue microarray (Figure 2). This TMA includes 158 stage III melanoma patients prospectively being followed for recurrence free survival, as well as 195 positive and negative controls and is being studied for scores of potential markers. Of these 158 patients, 86 underwent high dose IL-2 immunotherapy. The data analysis from this study is ongoing. The stained slides are sent to JWI where they are evaluated for overall and disease free survival. Using this TMA, we have confirmed that IL-24 does not independently correlate with patient survival. Evaluation of IL-2R beta staining is currently in process and statistics will be run to determine whether the presence of IL-2R beta alone or both IL-2R beta and IL-24 together correlate with prolonged patient survival. References • American Cancer Society Statistics 2007 • Grimm EA, et al, J Exp Med 1982;155:1823 • Atkins MB, et al, Cancer J Sci Am 2006; 6:S11 • Chada S, et al, Int Immunopharmacol 2004; 4:649 • Fisher PB, et al, Cancer Biol Ther 2003; 2:S23 Texas Pediatric Society Electronic Poster Contest Insert Program or Hospital Logo

![[Insert Hospital Name]](https://cdn0.slideserve.com/59021/insert-hospital-name-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/1968686/slide1-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/2208608/slide1-dt.jpg)