Download
1 / 55
560 likes | 922 Views
NEUROLYTIC BLOCKS. Dr.R.SILAMBAN MADRAS MEDICAL COLLEGE. NEUROLYTIC BLOCKS. Involves blocking of sympathetic chain at various levels Prevents transmission of pain impulses from the target organs to the brain. NEUROLYTIC BLOCKS. The nerves have the tendency to

E N D
NEUROLYTIC BLOCKS Dr.R.SILAMBAN MADRAS MEDICAL COLLEGE
NEUROLYTIC BLOCKS • Involves blocking of sympathetic chain at various levels • Prevents transmission of pain impulses from the target organs to the brain
NEUROLYTIC BLOCKS • The nerves have the tendency to regenerate • Blocking effect is temporary
DURATION • 3 months to 24 months
COMMON NEUROLYTIC BLOCKS • Stellate ganglion block • Thoracic sympathetic chain block • Coeliac plexus block • Lumbar sympathetic block • Superior hypogastric block • Ganglion impar block
STELLATE GANGLION BLOCK Stellate ganglion formed by union of • Middle cervical • Lower cervical • First thoracic segment
STELLATE GANGLION BLOCK Pain relief to structures of • Neck • Face • Upper limb • Upper thorax upto T5
THORACIC SYMPATHETIC CHAIN BLOCK • Not used widely • High risk of pneumothorax • Middle and lower thoracic region
LUMBAR SYMPATHETIC BLOCK • Needle introduced at the level of L2 or L2 + L4 • Pain relief to pelvis and lower limb • Volume required – 8 to 10ml
SUPERIOR HYPOGASTRIC PLEXUS BLOCK • From splenic flexure of colon to middle 3rd of rectum • Pain relief to pelvis and lower limb
SUPERIOR HYPOGASTRIC PLEXUS BLOCK • Most difficult block to perform • Needle has to enter through a small triangular space between iliac crest and transverse process of L5 • Volume required - 7ml for each side
GANGLION IMPAR BLOCK • Walther’s ganglion - lies in front of S2, S3 • Pain relief for lower rectum, anal canal and perineum including vulva and vagina
GANGLION IMPAR BLOCK • Patient in lithotomy or lateral position • Bent 10cm needle introduced in front of the coccyx • Finger inserted into rectum to guide the needle close to the sacral curvature • Volume required - 10ml
HISTORY 1914 – KAPPIS – first block in lateral position 1920 – WELDING – anterior approach. 1927 – LABAT – now followed retrocrural approach in prone position. 1982 – SINGLERS – CT guided transcrural approach 1983– ISCHIA – posterior transaortic approach
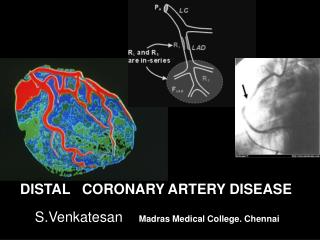
AREA OF SUPPLY • LOWER END OF ESOPHAGUS UPTO SPLENIC FLEXURE. • LIVER,SPLEEN • RETROPERITONEAL • STRUCTURES LIKE PANCREAS, KIDNEY.
INDICATIONS Chronic malignant & non malignant visceral pain 1. Upper g.i. malignancy 2. Chronic pancreatitis 3. Acute pancreatitis 4. Repeated abdominal surgeries 5. HIV related sclerosing cholangitis 6. Diagnostic purposes 7. Abdominal angina
ROLE IN CHRONIC PANCREATITIS Controversial Useful in • Few selected cases • Acute exacerbations
ROLE IN ACUTE PANCREATITIS • Steroids improved morbidity and mortality • Continuous infusion for pain relief
CONTRAINDICATIONS ABSOLUTE • Anti coagulant therapy • Coagulopathy • Anti-blastic cancer therapy • Bowel obstruction • Patient on disulfuram therapy
CONTRAINDICATION RELATIVE • Drug seeking behaviour to pain • Patient on CNS depressant drugs
TECHNIQUE Posterior approach Anterior approach • Retrocrural • Antecrural • transaortic
RETROCRURAL APPROACH • Bilateral Posterior approach • Splanchnic block • Drug deposited behind the crus of diaphragm
ANTECRURAL APPROACH • Unilateral approach • Right sided only • Needle placed anterior to • crus of diaphragm.
COMPLICATIONS MINOR • HYPOTENSION • POSTURAL HYPOTENSION • DIARRHEA • PAIN • CHEMICAL COMPLICATIONS
COMPLICATIONS CHEMICAL ALCOHOL FACIAL FLUSHING, PALPITATIONS, DIAPHORESIS PHENOL TRANSIENT TINNITUS, FLUSHING,MALAISE CNS STIMULATION, MYOCLONUS, SEIZURES,HYPERTENSION,ARRYTHMIAS,HEPATIC &RENAL INSUFFICIENCY
COMPLICATIONS • VISCERAL INJURY • EJACULATION FAILURE • NERVE ROOT INJURY MODERATE
COMPLICATION MAJOR • PARAPLEGIA • LUNG INJURY • VASCULAR TRAUMA • EPIDURAL & SUB ARACHNOID INJECTION
EFFICACY OF COELIACPLEXUS BLOCK Controversy Regarding • Efficacy relative to opioid therapy • Efficacy relative to various approaches • Comittment to neurolysis despite remote risk of paraplegia
ADVANTAGE OF COELIAC PLEXUS NEUROLYSIS • Better long term pain relief • Decrease drug dose for maintainance • Better quality of life • Improved performance status • Overcomes the G.I.T effects of opioids • In weight and survival rate
FAILURE DUE TO • Delayed application • Tumour extension • Poor technique
DRUGS • ALCOHOL • PHENOL • LOCAL ANAESTHETICS
ALCOHOL • COMMONLY USED • HYPOBARIC • CEPHALAD SPREAD RADIOGRAPHICALLY • USED IN CONCENTRATION OF 50-100% • VOLUME REQUIRED-40 ml
ALCOHOL ADVANTAGES • LONGER DURATION OF ACTION • EASILY AVAILABLE • IMMEDIATE NEUROLYSIS • PAIN ON INJECTION CONFIRMS CORRECT PLACEMENT IN THE BLIND APPROACH • LESS AFFINITY FOR VASCULAR TISSUES
ALCOHOL DISADVANTAGES • PAIN ON INJECTION • CANNOT BE COMBINED WITH DYE
PHENOL • HYPERBARIC • CAUDAL SPREAD RADIOGRAPHICALLY • 7.5 – 10% SOLUTION PREFFERED • MAXIMUM DOSE – 40 mg/kg