Download
1 / 42
510 likes | 1.05k Views
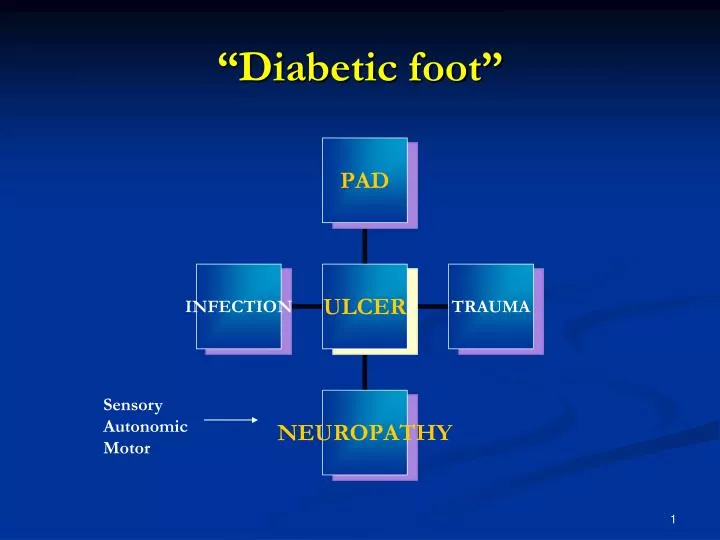
“Diabetic foot”. Sensory Autonomic Motor. Diabetic foot ulceration. Neuropathic: 45-60% Purely ischaemic: 10% Mixed neuroischaemic: 25-40%. Diabetes and PAD Spectrum of disease. Intermittent claudication Rest pain Ulceration/gangrene Incidental/Screening. Intermittent claudication.

E N D
“Diabetic foot” Sensory Autonomic Motor
Diabetic foot ulceration • Neuropathic: 45-60% • Purely ischaemic: 10% • Mixed neuroischaemic: 25-40%
Diabetes and PADSpectrum of disease • Intermittent claudication • Rest pain • Ulceration/gangrene • Incidental/Screening
Intermittent Claudication • Prevalence: 5.3% in patients aged 45-74yrs • Quality of life: Significantly impaired • Limb Outlook: Relatively benign 10% require intervention to prevent limb loss 1% per year require amputation • Life expectancy: 2-4 X ↑ mortality
Peripheral Arterial Disease and All-Cause Mortality 1.00 Normal subjects 0.75 Asymptomatic PAD† 0.50 Survival Symptomatic PAD† 0.25 Severe symptomatic PAD† 0.00 0 2 4 6 8 10 12 Year • *Kaplan-Meier survival curves based on mortality from all causes • †Large-vessel PAD • 1. Criqui MH. Vasc Med 2001; 6(suppl 1): 3–7.
Odds ratio for risk factors for intermittent claudication Odds Ratio Protective Harmful -2 -1 0 1 2 3 4 Male gender (cf female) Age (per 10 years) Diabetes Smoking Hypertension Hypercholesterolemia Fibrinogen Alcohol Dormandy JA et al. J Vasc Surgery. 2000;31(1 Part 2):S1-S296.
Intermittent Claudicationand diabetes • Prevalence: 2 x ↑ • Diabetics – 20% of PAD population • Limb Outlook: Worse • 2x ↑ rest pain, 6x ↑gangrene • 80% of amputations occur in diabetics • Life expectancy: 8 x ↑ mortality
Diagnosis: History • Intermittent claudication cramp like pain in muscles Location: buttock, thigh, calf ,foot occurs on exercising relieved by rest • Atypical symptoms are common
Diagnosis – clinical examination • Examination of pulses Peripheral pulses- HIGHLY SUBJECTIVE • Rotterdam study 60% inaccurate
Pulses & PAD • Collins 206, 403 pts screened • PAD prevalence :16.6% • Sensitivity of a non detectable pedal pulse -18% • Specificity: 98% • Post tibial pulse: sensitivity 33%, specificity 66% ( Brealey S et al) • Probability of agreement of an absent pedal pulse between experienced examiners : 0.49-0.59 (Marinelli et al)
Ankle pressure (mm Hg) Brachial pressure (mm Hg) ABPI = Ankle Brachial Pressure Index (ABPI) Value <0.9 indicates PAD
Figure 1.5 ABPI – DIAGNOSIS & PROGNOSIS McKenna et al, atherosclerosis, 1991
ABPI • Reliable • Positive predictive value -95% • Negative predictive value-99% • But a normal ABPI at rest and classical symptoms may indicate need for exercise ABPI • ESSENTIAL FOR DIAGNOSIS • Do we have expertise in the community?
Diabetes and ABPI • Medial calcification: non compressible (nc) arteries • ABPI in diabetics : 5-10% too high • Alternatives: Elevate foot Toe pressures
Toe pressures • Cuff placed around proximal phalanx • Normal pressures are less than ankle pressures • average 24± 7 – 41± 17mmHg • Normal ratios compared to brachial 0.72-0.91
CLAUDICATION: SURGICAL TREATMENT • First line : Prolong life Risk factor management • Improve symptoms Exercise Medical therapy Revascularisation
Treatment • *Statin for all • *Screen for diabetes/ Glycaemic control • *BP control • Smoking cessation: NRT • Anti-platelet therapy • Increase exercise • ACE inhibitor (HOPE study) • Review: ? For revascularisation
VASCULAR EVENT by PRIOR DISEASE MRC/BHF Heart Protection Study STATIN worse Baseline STATIN PLACEBO Risk ratio and 95% CI feature (10269) (10267) STATIN better STATIN worse Previous MI 1007 1255 Other CHD (not MI) 452 597 No prior CHD CVD 182 215 PVD 332 427 Diabetes 279 369 ALL PATIENTS 2042 2606 24% SE 2.6 reduction (19.9%) (25.4%) (2P<0.00001) 0.4 0.6 0.8 1.0 1.2 1.4
Diabetes and PAD • No clinical trials have been set up specifically to investigate glycaemic control. • Type 2 diabetes, glycaemia (HbA1C) risk of cardiovascular morbidity and mortality (1) • Each 1% difference in HbA1C 21% (95% CI 15-27%) change in the risk of diabetes-related death and a 14% reduction in fatal and nonfatal myocardial infarction over 10 years (2) Turner RC, et al.. BMJ 1998; 316: 823-8. Stratton IM et al,. BMJ. 2000;321(7258):405-12.
HOPE study • Effects of ramipril on patients with 1. symptomatic PAD 2. Asymptomatic PAD (ABPI≤ 0.9) plus an additional coronary risk factor were analysed. • Only 50% of the patients were defined as hypertensive. • In both groups- ~ 25% reduction in the primary combined outcome of cardiovascular mortality, myocardial infarction or stroke with ramipril. • (ABPI) was measured unconventionally Ostergren J, et al. Eur Heart J 2004; 25: 17-24.
Diabetes and PADSpectrum of disease • Intermittent claudication • Rest pain • Ulceration/gangrene • Incidental/Screening
Severe limb ischaemia Rest pain>2/52, Tissue loss ABPI <0.5
Severe limb ischaemia Rest pain>2/52, Tissue loss ABPI <0.5 Critical limb ischaemia Absolute ankle pressure <50mmHg
Diabetic foot ulceration • Neuropathic: 45-60% • Purely ischaemic: 10% • Mixed neuroischaemic: 25-40%
Diabetes & foot ulcers • 15% develop a foot ulcer • 12-24% require amputation • Leading cause of lower limb amputation
Will the ulcer heal? Study of patients with foot ulcers and toe amputations Non-heeling occurred in(Ramsey et al) • 92% of limbs with ankle pressure <80mmHg • But also in 45% of limbs with higher ankle pressures • 95% of limbs with toe pressures <30mmHg • But only in 14% of limbs with higher toe pressures • Toe pressures – greater prognostic value • PPV 67%, NPV 77% (Kaloni et al, 1999;Diabetes Care)
Investigation of PAD in patients with diabetes • Duplex scan • Angiography • CT angiography • MRA/MRI
Figure 1.2 Figure 1.2 A B C D
Diabetes: distribution of PAD • Atherosclerosis in : • Classical sites: aorto-iliac, Fem artery • Medium-sized vessels- peroneal/tibial vessels Foot vessels spared
Revascularisation • Angioplasty • By-pass
Figure 3.8 Figure 3.8
Amputation • Minor- infection, osteomyelitis Possible if good blood supply • Major – extensive soft tissue infection or Insufficient blood supply • 80% of amputees have diabetes
When to refer ? • Symptoms: Intermittent claudication Rest pain ( nb neuropathy) • Signs: low/nc ABPIs Ulceration Gangrene • ? ? Screening – value for risk factor Mx
Asymptomatic PAD • Relatively common • Associated with increased mortality • Can early treatment prevent events ? 2 Major trials will report ‘06/’07 • Potential to save lives using ABPI: a simplenon-invasive screening test
£ British Heart Foundation Study Population: men and women >50 years of age Endpoints Cardiovascular• Events• Deaths Aspirin vs placebo Aspirin for Asymptomatic Atherosclerosis (AAA) Trial ABPI<0.95 N=3334 3- 4 YearFollow-up Fowkes & Douglas, personal communication 2002
Royal Collegeof Physicians Diabetic Registry Group Low ABPI in 20.1% Endpoints Cardiovascular• Events• Deaths £ Medical Research Council POPADAD ABPI <0.99Diabetes Men & women aged>40 yearsN=8000 NO clinical evidence of vascular disease