Download

1 / 34
360 likes | 403 Views
Malignant Hyperthermia. Catherine Maw 24/10/2012. OUTLINE. Define and discuss aetiology of thermal disorders Relevance to ICU Clinical Presentation of MH Differential diagnosis and pitfalls Treatment in theatre and ICU Subsequent management. Thermoregulation.

E N D
Malignant Hyperthermia Catherine Maw 24/10/2012
OUTLINE • Define and discuss aetiology of thermal disorders • Relevance to ICU • Clinical Presentation of MH • Differential diagnosis and pitfalls • Treatment in theatre and ICU • Subsequent management
Thermoregulation • Balance between heat production and loss • Hypothalamic thermoregulatory centre • “Pyrexia” = resetting of thermoregulatory set point to a higher level by activation of heat conserving mechanisms • “Hyperthermia” = failure of effector mechanisms to maintain the normal set point
Fever in the ICU • Regulated hyperthermia • Endogenous pyrogens (IL6 and PGE2) act on the hypothalamus • Reset the thermoregulatory set point to higher temp • Effector organs prevent heat loss • May be protective • When pyrogens decrease, set point decreases • Deleterious effects (↑CO, O2 consumption, CO2 production)
Hyperthermia • Failure of effector mechanisms to maintain the hypothalamic set point (core ≥ 40°C) • Heat stroke • Drug induced hyperthermias (MH, NMS, Serotonin syndrome, sympathomimetic syndrome, anticholinergic syndrome) • Heat injury is the insult • Protein denaturation and lipid dissolution at 42°C (core)
Why is it fatal? • Direct cellular damage • Increases membrane permeability • Activation of Na-K-ATPase pump • ATP depletion • Tissue oedema • Cytokine activation, coagulation cascade activation • Cellular death (lactate, hyperkalaemia, acidosis) • Similar picture to sepsis
Why? • Metabolic acidosis • Hyperkalaemia • Rhabdomyolysis • Renal failure • DIC • Liver failure • Death
Australian History • 1960: Dr Jim Villiers at Royal Melbourne Hospital • Patient with 10 family members who died under GA • Patient had malignant hyperthermia (MH) • Villiers presented the successful anaesthetic outcome • 1972: Lancet. Denborough and Lovell. • Royal Melbourne (one of 3) centres for MH
Definition and Aetiology • Pharmacological disease of skeletal muscle • Hypermetabolic crisis • Induced by exposure to volatile anaesthetic agents or Suxamethonium • Loss of normal calcium homeostasis • Unregulated release of Calcium form the sarcoplasmic reticulum • Myocytehypermetabolism
Relevance • Anaesthetic complication • Ongoing patient care will always involve ICU • Insidious versus acute • True MH rare • Hyperthermia differentials more common
Epidemiology • 1 in 10,000 to 1 in 30,000 anaesthetics • Young adults (45-55% of cases in <19 years) • More frequent in minor ops • Male > Female 2:1 • Mortality previously 70-80% • Reduced to 2-3% now
Geneticsof MH • Majority of MH susceptible patients have mutations on RYR1 or DHP genes • Inherited or spontaneous • 50% Autosomal Dominant • 200 mutations identified • 29 have causality
Pathophysiology ctd • Sustained muscle contraction due to high levels of myoplasmic calcium • Heat generated (initial insult) • Cascade similar to sepsis/systemic inflammation • Initial aerobic metabolism generating CO2 and → cellular acidosis • Then Oxygen and ATP depletion → worsening acidosis and lactate production • Depleted energy → muscle death and rhabdomyolysis
Risk Factors • Positive family history • Previous exposure to Suxamethonium or volatiles • Exertional heat stroke • Exercise induced rhabdomyolysis • Central core disease • Scoliosis • Strabismus surgery
Early • Prolonged masseter muscle spasm after Suxamethonium • Inappropriately ↑ ETCO2 or tachypnoea during spontaneous respiration (ETCO2 >60) • Inappropriately ↑ ETCO2 (ETCO2 >55) during controlled ventilation • Inappropriate tachycardia • Cardiac arrhythmias, especially ventricular ectopics
Developing • Developing rise in temperature (0.5 ◦C per 15 mins) • Progressive respiratory and later metabolic acidosis • Hyperkalaemia • Profuse sweating • Cardiovascular instability • Desaturation • Generalised muscle rigidity
Late • Myoglobinuria • Myalgia • Grossly elevated CK • Coagulopathy • Cardiac arrest
Differential diagnosis • Inadequate anaesthesia / machine issue / patient factor • Sepsis • Intracerebral infection or bleed • Recreational drugs • Neuroleptic malignant syndrome • Thyroid storm • Phaeochromocytoma
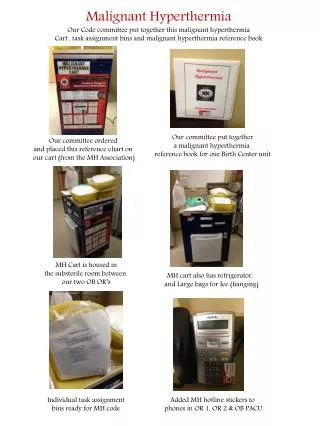
Management • ANZCA suggest MH Resource kit • Link to mhanz • Task cards based on the aviation safety model • If diagnosis is suspected: • Declare Emergency • Call for HELP and send for MH resource kit • Turn off the volatile and remove vaporisers • Hyperventilate on >15l/min fresh gas flows with 100% O2 • TIVA
Ongoing Care • ICU for ventilatory support, haemodynamic monitoring, renal support • CK peaks at 14 hours • Dantrolene does not effect cardiac or smooth muscle • Recrudescence in 25% • 1mg/kg Dantrolene every 6 hours for 48 hours
MH Susceptibility Testing • Gold standard is the contracture test • In vitro response of a fresh sample of muscle tissue to Caffeine or Halothane • Muscle strip in physiological solution is attached to a strain gauge and electrically stimulated to measure baseline tension • Repeat in Halothane and Caffeine • High sensitivity and specificity • Expensive and specialist referral needed • Genetic testing cheaper but sensitivity 30-50%