Download
1 / 1
10 likes | 125 Views
Collaborating to develop a disease prevention program for a hard-to-reach population Amy B. Jessop , PhD, MPH 1,5 , Jerome Wells , MS 2 , Monika Burke , RN, MPH 1,4 , Kate Cushman , MPH 3 , John Muccitelli , RN,MPH 1

E N D
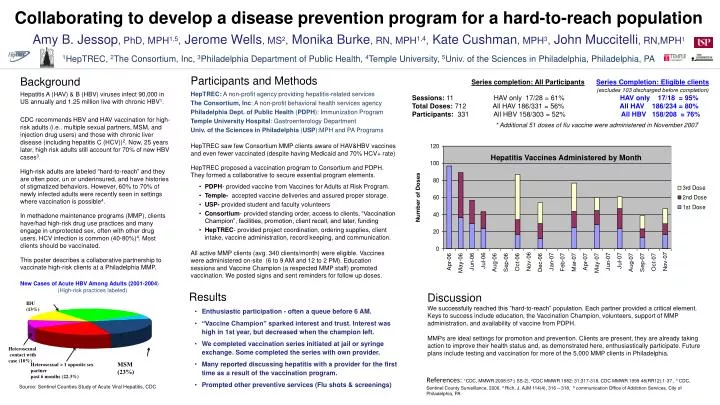
Collaborating to develop a disease prevention program for a hard-to-reach population Amy B. Jessop, PhD, MPH1,5,Jerome Wells, MS2,Monika Burke, RN,MPH1,4,Kate Cushman, MPH3,John Muccitelli, RN,MPH1 1HepTREC, 2The Consortium, Inc, 3Philadelphia Department of Public Health, 4Temple University, 5Univ. of the Sciences in Philadelphia, Philadelphia, PA • Participants and Methods • HepTREC: A non-profit agency providing hepatitis-related services • The Consortium, Inc: A non-profit behavioral health services agency • Philadelphia Dept. of Public Health (PDPH): Immunization Program • Temple University Hospital: Gastroenterology Department • Univ. of the Sciences in Philadelphia (USP):MPH and PA Programs • HepTREC saw few Consortium MMP clients aware of HAV&HBV vaccines and even fewer vaccinated (despite having Medicaid and 70% HCV+ rate) • HepTREC proposed a vaccination program to Consortium and PDPH. They formed a collaborative to secure essential program elements. • PDPH- provided vaccine from Vaccines for Adults at Risk Program. • Temple- accepted vaccine deliveries and assured proper storage. • USP- provided student and faculty volunteers • Consortium- provided standing order, access to clients, “Vaccination Champion”, facilities, promotion, client recall, and later, funding • HepTREC- provided project coordination, ordering supplies, client intake, vaccine administration, record keeping, and communication. • All active MMP clients (avg. 340 clients/month) were eligible. Vaccines were administered on-site (6 to 9 AM and 12 to 2 PM). Education sessions and Vaccine Champion (a respected MMP staff) promoted vaccination. We posted signs and sent reminders for follow up doses. Background Hepatitis A (HAV) & B (HBV) viruses infect 90,000 in US annually and 1.25 million live with chronic HBV1. CDC recommends HBV and HAV vaccination for high-risk adults (i.e.. multiple sexual partners, MSM, and injection drug users) and those with chronic liver disease (including hepatitis C (HCV))2. Now, 25 years later, high risk adults still account for 70% of new HBV cases3. High-risk adults are labeled “hard-to-reach” and they are often poor, un or underinsured, and have histories of stigmatized behaviors. However, 60% to 70% of newly infected adults were recently seen in settings where vaccination is possible4. In methadone maintenance programs (MMP), clients have/had high-risk drug use practices and many engage in unprotected sex, often with other drug users. HCV infection is common (40-80%)4. Most clients should be vaccinated. This poster describes a collaborative partnership to vaccinate high-risk clients at a Philadelphia MMP. Series completion: All ParticipantsSeries Completion: Eligible clients (excludes 103 discharged before completion) Sessions: 11 HAV only 17/28 = 61% HAV only 17/18 = 95% Total Doses: 712 All HAV 186/331 = 56% All HAV 186/234 = 80% Participants: 331 All HBV 158/303 = 52% All HBV 158/208 = 76% * Additional 51 doses of flu vaccine were administered in November 2007 Hepatitis Vaccines Administered by Month New Cases of Acute HBV Among Adults (2001-2004) (High-risk practices labeled) • Results • Enthusiastic participation - often a queue before 6 AM. • “Vaccine Champion” sparked interest and trust. Interest was high in 1st year, but decreased when the champion left. • We completed vaccination series initiated at jail or syringe exchange. Some completed the series with own provider. • Many reported discussing hepatitis with a provider for the first time as a result of the vaccination program. • Prompted other preventive services (Flu shots & screenings) Discussion We successfully reached this “hard-to-reach” population. Each partner provided a critical element. Keys to success include education, the Vaccination Champion, volunteers, support of MMP administration, and availability of vaccine from PDPH. MMPs are ideal settings for promotion and prevention. Clients are present, they are already taking action to improve their health status and, as demonstrated here, enthusiastically participate. Future plans include testing and vaccination for more of the 5,000 MMP clients in Philadelphia. IDU (13%) Heterosexual contact with case (10%) MSM (23%) Heterosexual > 1 opposite sex partner past 6 months (22.3%) References:1CDC, MMWR 2008:57;( SS-2), 2CDC MMWR 1982: 31;317-318, CDC MMWR 1999 48(RR12);1-37 , 3 CDC, Sentinel County Surveillance, 2006. 4 Rich, J. AJM 114(4), 316 – 318, 5 communication Office of Addiction Services, City of Philadelphia, PA Source: Sentinel Counties Study of Acute Viral Hepatitis, CDC