Download
1 / 1
10 likes | 80 Views
Racial Disparities in the Prevalence of Medical Home for Children with Asthma in Alabama Julianna Bailey, RD, LaKiesha Bonham, RRT, Bridget Cobb, MSW, Casey Voorhees, MSW, MPH UAB Pediatric Pulmonary Center, Birmingham, Alabama. INTRODUCTION. CONCLUSIONS. RESULTS.

E N D
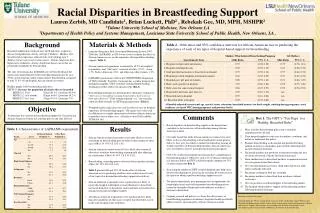
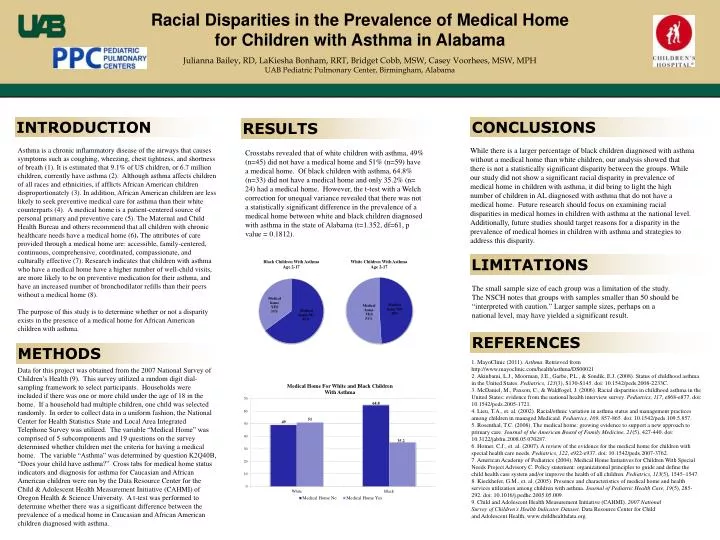
Racial Disparities in the Prevalence of Medical Home for Children with Asthma in Alabama Julianna Bailey, RD, LaKiesha Bonham, RRT, Bridget Cobb, MSW, Casey Voorhees, MSW, MPH UAB Pediatric Pulmonary Center, Birmingham, Alabama INTRODUCTION CONCLUSIONS RESULTS Asthma is a chronic inflammatory disease of the airways that causes symptoms such as coughing, wheezing, chest tightness, and shortness of breath (1). It is estimated that 9.1% of US children, or 6.7 million children, currently have asthma (2). Although asthma affects children of all races and ethnicities, if afflicts African American children disproportionately (3). In addition, African American children are less likely to seek preventive medical care for asthma than their white counterparts (4). A medical home is a patient-centered source of personal primary and preventive care (5). The Maternal and Child Health Bureau and others recommend that all children with chronic healthcare needs have a medical home (6). The attributes of care provided through a medical home are: accessible, family-centered, continuous, comprehensive, coordinated, compassionate, and culturally effective (7). Research indicates that children with asthma who have a medical home have a higher number of well-child visits, are more likely to be on preventive medication for their asthma, and have an increased number of bronchodilator refills than their peers without a medical home (8). The purpose of this study is to determine whether or not a disparity exists in the presence of a medical home for African American children with asthma. While there is a larger percentage of black children diagnosed with asthma without a medical home than white children, our analysis showed that there is not a statistically significant disparity between the groups. While our study did not show a significant racial disparity in prevalence of medical home in children with asthma, it did bring to light the high number of children in AL diagnosed with asthma that do not have a medical home. Future research should focus on examining racial disparities in medical homes in children with asthma at the national level. Additionally, future studies should target reasons for a disparity in the prevalence of medical homes in children with asthma and strategies to address this disparity. Crosstabs revealed that of white children with asthma, 49% (n=45) did not have a medical home and 51% (n=59) have a medical home. Of black children with asthma, 64.8% (n=33) did not have a medical home and only 35.2% (n= 24) had a medical home. However, the t-test with a Welch correction for unequal variance revealed that there was not a statistically significant difference in the prevalence of a medical home between white and black children diagnosed with asthma in the state of Alabama (t=1.352, df=61, p value = 0.1812). LIMITATIONS The small sample size of each group was a limitation of the study. The NSCH notes that groups with samples smaller than 50 should be “interpreted with caution.” Larger sample sizes, perhaps on a national level, may have yielded a significant result. REFERENCES METHODS 1. MayoClinic (2011). Asthma. Retrieved from http://www.mayoclinic.com/health/asthma/DS00021 2. Akinbami, L.J., Moorman, J.E., Garbe, P.L., & Sondik, E.J. (2008). Status of childhood asthma in the United States. Pediatrics, 123(3), S130-S145. doi: 10.1542/peds.2008-2233C. 3. McDaniel, M., Paxson, C., & Waldfogel, J. (2006). Racial disparities in childhood asthma in the United States: evidence from the national health interview survey. Pediatrics, 117, e868-e877. doi: 10.1542/peds.2005-1721. 4. Lieu, T.A., et. al. (2002). Racial/ethnic variation in asthma status and management practices among children in managed Medicaid. Pediatrics, 109, 857-865. doi: 10.1542/peds.109.5.857. 5. Rosenthal, T.C. (2008). The medical home: growing evidence to support a new approach to primary care. Journal of the American Board of Family Medicine, 21(5), 427-440. doi: 10.3122/jabfm.2008.05.070287. 6. Homer, C.J., et. al. (2007). A review of the evidence for the medical home for children with special health care needs. Pediatrics, 122, e922-e937. doi: 10.1542/peds.2007-3762. 7. American Academy of Pediatrics (2004). Medical Home Initiatives for Children With Special Needs Project Advisory C. Policy statement: organizational principles to guide and define the child health care system and/or improve the health of all children. Pediatrics, 113(5), 1545–1547. 8. Kieckhefer, G.M., et. al. (2005). Presence and characteristics of medical home and health services utilization among children with asthma. Journal of Pediatric Health Care, 19(5), 285-292. doi: 10.1016/j.pedhc.2005.05.009. 9. Child and Adolescent Health Measurement Initiative (CAHMI). 2007 National Survey of Children’s Health Indicator Dataset. Data Resource Center for Child and Adolescent Health, www.childhealthdata.org. Data for this project was obtained from the 2007 National Survey of Children’s Health (9). This survey utilized a random digit dial-sampling framework to select participants. Households were included if there was one or more child under the age of 18 in the home. If a household had multiple children, one child was selected randomly. In order to collect data in a uniform fashion, the National Center for Health Statistics State and Local Area Integrated Telephone Survey was utilized. The variable “Medical Home” was comprised of 5 subcomponents and 19 questions on the survey determined whether children met the criteria for having a medical home. The variable “Asthma” was determined by question K2Q40B, “Does your child have asthma?” Cross tabs for medical home status indicators and diagnosis for asthma for Caucasian and African American children were run by the Data Resource Center for the Child & Adolescent Health Measurement Initiative (CAHMI) of Oregon Health & Science University. A t-test was performed to determine whether there was a significant difference between the prevalence of a medical home in Caucasian and African American children diagnosed with asthma.