Download
1 / 28
280 likes | 414 Views
Health Insurance Exchanges. This presentation is a high-level summary and for general informational purposes only. The information in this presentation is not comprehensive and does not constitute legal, tax, compliance or other advice or guidance. Exchange Overview Topics. Plans & Benefits.

E N D
Health Insurance Exchanges This presentation is a high-level summary and for general informational purposes only. The information in this presentation is not comprehensive and does not constitute legal, tax, compliance or other advice or guidance.
Exchange Overview Topics Plans & Benefits Definitions, Functions & Models Credits and subsidies SHOP Timeline
Exchanges Defined The Affordable Care Act authorizes states to create and operate exchanges, also known as health insurance marketplaces, for individuals and for small business employers by 2014. A federal exchange will be available if a state does not have its own exchange. • Designed to be competitive and centralized online sites for individuals to purchase health insurance plans. • Meant to help people meet ACA’s minimum coverage requirement (also called the individual mandate). • Intended to provide unbiased, “non-marketing” information to help consumers better understand the options available to them and choose a plan.
What are Exchanges? • Think Catalog Shopping Online Health insurance exchanges are the online sites where individuals and small business owners can shop health care plans offered by various insurance carriers.
Exchange Functions 1 5 2 4 3 7 6 Run websites that allow consumers to shop for qualified health plans Help consumers and employers choose & enroll in coverage Inform consumers about individual mandate exemptions PublicExchanges Provide toll-free hotline for assistance & other avenues for customer service Determine eligibility for a QHP, Medicaid, CHIP & enroll if eligible Help eligible individuals getfederal tax credits & subsidies Perform Risk Adjustment
Consumer Support Consumers Navigators Brokers Direct Public Exchange
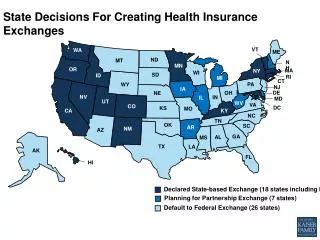
Exchange Models • A state may choose to establish and operate its exchange, which is called a STATE-BASED model. • A state may decide to implement an exchange operated by both the state and Health and Human Services (HHS), also called a STATE PARTNERSHIP model. • If a state does not submit an exchange blueprint to HHS, or if HHS finds the state is not exchange-ready, then HHS will operate a FEDERALLY FACILITATED model for that state.
Four Benefit Levels of Coverage • The key difference between the “metallic” plans is the expected percentage of medical expenses shared between the health plan and the member. Platinum Gold Silver Bronze Expected Percentage of Medical Expenses Covered by the Health Plan Expected Percentage of Medical Expenses Covered by the Member
Qualified Health Plans A Qualified Health Plan (QHP) is a health insurance plan that has been certified to be allowed for purchase on an individual exchange and SHOP. • Only certified QHPs are allowed on an individual exchange and SHOP. • HHS established the criteria for how to certify a QHP. Several things must happen. The product must: • Get certified by the exchange (QHP certification). • Provide essential health benefits (EHB) that meet state and federal guidelines. • Follow established limits on cost-sharing (such as deductibles and copayments). • Meet provider network adequacy rules.
Essential Health Benefits In 2014, individual and small group plans on and off the exchange must include Essential Health Benefits, which are generally services and items in the following 10 benefit categories: Maternity and newborn care Mental health, substance abuse disorder services,behavioral health treatment Hospitalization Emergency services Laboratory services Prescription drugs Ambulatory patient services Habilitative and rehabilitative services and devices Preventive and wellness services and chronic disease management Pediatric services, including oral and vision care 12
Benchmark Plans • A benchmark plan serves as a state’s reference health plan of essential health benefits (EHB). • Each state needed to select a health insurance plan currently operating within the state to act as the benchmark plan. Default Benchmark • If a state did not select a benchmark, HHS determined that the EHB benchmark defaulted to the largest (by enrollment) small-group plan in the state. EHBs and Benchmark Plans
EHB Benchmark for Illinois* Filling in the 10 EHB Categories • ACA tasked HHS to define EHB details • HHS proposed a state-specific benchmark approach • Each state was asked to select a benchmark plan • States had until Dec. 26, 2012 to submit a plan to represent the state’s version of EHBs for 2014 and 2015 plan years • Default choice for states that did not select a plan: The state’s largest small group health plan • HHS released a proposed rule on EHBs, Actuarial Value (AV) and Accreditation in late November 2012. It was open for comment until Dec. 2012. • HHS released final rule on Feb. 20, 2013 along with FAQs on ACA Implementation about cost-sharing limits related to EHBs. *Source: http://cciio.cms.gov/resources/EHBBenchmark/illinois-ehb-benchmark-plan.pdf Resources • HHS final rule: http://www.gpo.gov/fdsys/pkg/FR-2013-02-25/pdf/2013-04084.pdf • Center for Consumer Information & Insurance Oversight http://cciio.cms.gov/resources/factsheets/ehb-2-20-2013.html • EHB benchmark plans for 50 states http://cciio.cms.gov/resources/data/ehb.html
EHB Benchmark for New Mexico* Filling in the 10 EHB Categories • ACA tasked HHS to define EHB details • HHS proposed a state-specific benchmark approach • Each state was asked to select a benchmark plan • States had until Dec. 26, 2012 to submit a plan to represent the state’s version of EHBs for 2014 and 2015 plan years • Default choice for states that did not select a plan: The state’s largest small group health plan • HHS released a proposed rule on EHBs, Actuarial Value (AV) and Accreditation in late November 2012. It was open for comment until Dec. 2012. • HHS released final rule on Feb. 20, 2013 along with FAQs on ACA Implementation about cost-sharing limits related to EHBs. *Source: http://cciio.cms.gov/resources/EHBBenchmark/new-mexico-ehb-benchmark-plan.pdf Resources • HHS final rule: http://www.gpo.gov/fdsys/pkg/FR-2013-02-25/pdf/2013-04084.pdf • Center for Consumer Information & Insurance Oversight http://cciio.cms.gov/resources/factsheets/ehb-2-20-2013.html • EHB benchmark plans for 50 states http://cciio.cms.gov/resources/data/ehb.html
EHB Benchmark for Oklahoma* Filling in the 10 EHB Categories • ACA tasked HHS to define EHB details • HHS proposed a state-specific benchmark approach • Each state was asked to select a benchmark plan • States had until Dec. 26, 2012 to submit a plan to represent the state’s version of EHBs for 2014 and 2015 plan years • Default choice for states that did not select a plan: The state’s largest small group health plan • HHS released a proposed rule on EHBs, Actuarial Value (AV) and Accreditation in late November 2012. It was open for comment until Dec. 2012. • HHS released final rule on Feb. 20, 2013 along with FAQs on ACA Implementation about cost-sharing limits related to EHBs. *Source: http://cciio.cms.gov/resources/EHBBenchmark/oklahoma-ehb-benchmark-plan.pdf Resources • HHS final rule: http://www.gpo.gov/fdsys/pkg/FR-2013-02-25/pdf/2013-04084.pdf • Center for Consumer Information & Insurance Oversight http://cciio.cms.gov/resources/factsheets/ehb-2-20-2013.html • EHB benchmark plans for 50 states http://cciio.cms.gov/resources/data/ehb.html
EHB Benchmark for Texas* Filling in the 10 EHB Categories • ACA tasked HHS to define EHB details • HHS proposed a state-specific benchmark approach • Each state was asked to select a benchmark plan • States had until Dec. 26, 2012 to submit a plan to represent the state’s version of EHBs for 2014 and 2015 plan years • Default choice for states that did not select a plan: The state’s largest small group health plan • HHS released a proposed rule on EHBs, Actuarial Value (AV) and Accreditation in late November 2012. It was open for comment until Dec. 2012. • HHS released final rule on Feb. 20, 2013 along with FAQs on ACA Implementation about cost-sharing limits related to EHBs. *Source: http://cciio.cms.gov/resources/EHBBenchmark/texas-ehb-benchmark-plan.pdf Resources • HHS final rule: http://www.gpo.gov/fdsys/pkg/FR-2013-02-25/pdf/2013-04084.pdf • Center for Consumer Information & Insurance Oversight http://cciio.cms.gov/resources/factsheets/ehb-2-20-2013.html • EHB benchmark plans for 50 states http://cciio.cms.gov/resources/data/ehb.html
Those with household incomes of 100-400% of FPL may be eligible to receive tax credits and subsidies. A family of 4 with a household income of $94,200 or less maybe eligible to receive premium tax credits. 2013 poverty guidelines for 48 contiguous states and the District of Columbia Understanding FPL Federal Poverty Levels SOURCE: 2013 HHS Poverty Guidelines published by the U.S. Department of Health and Human Services at http://aspe.hhs.gov/poverty/13poverty.cfm
Tax Credits & Subsidies for Individuals Premium Tax Credits • A tax credit is available based on a household income of 100-400% of the federal poverty level (FPL). The tax credit can be applied to a plan at any metallic level. It is advanceable. Note that premium tax credits are on a sliding scale. Out-of-Pocket Maximum Subsidy • An out-of-pocket maximum subsidy is available to those who select a silver plan and have an income of 100-400% of the FPL. Cost-Sharing Subsidy • A cost-sharing subsidy is available to those who select a silver plan and have an income of 100-250% of the FPL.
Beginning in 2014, citizens and legal residents must have and maintain a minimum level of health coverage or pay a federal tax. Taxes are assessed according to percentage of income or flat fee, whichever is greater, and will be applied on federal income tax returns. Penalties for the Uninsured Some individuals may qualify for an exemption from the requirement to carry insurance coverage.
Employee Choice* Hybrid Choice Small Business Health Options Program SmallBusinessHealthOptionsProgram (SHOP) SHOP is an online exchange where small employers (1-50 employees in 2014, 1-100 beginning 2016) can obtain health coverage for their employees, and possibly take advantage of tax credits. States will have the flexibility to determine who selects the coverage Employer Choice Employer may be permitted to select one or more specific plan on behalf of employees, or self Employer can select metallic level and then employee can select any plan (from any carrier) within that level Employee can select any plan offered, as long as it meets SHOP benefit plan design requirements
Tax Credits for Small Businesses The Affordable Care Act also establishes a Small Business Tax Credit that will help make offering health coverage more affordable for qualified small businesses. Now Beginning 2014 • Available to employers with fewer than 25 full time employees, with average annual wages less than $50,000 • Employers must contribute a uniform percentage of at least 50% toward their employee's insurance • Worth up to 35% of employer contributions to employees' health insurance plan (25% for nonprofit organizations. • Available to qualified employers that provide coverage to their employees on SHOP • Credits increase to up to 50% of the employer's contributions (35% for non-profit organizations)
Individual and SHOP Comparison Differences between individual exchanges and SHOP: