Download
1 / 41
410 likes | 532 Views
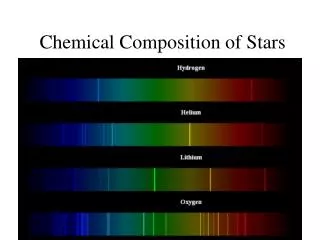
I. General Description of Enzymes A. Chemical composition 1 . Enzymes are proteins, compounds of high molecular weight, containing Carbon (C), hydrogen (H), oxygen (O), sulfur (S), nitrogen (N)

E N D
I. General Description of Enzymes A. Chemical composition 1. Enzymes are proteins, compounds of high molecular weight, containing Carbon (C), hydrogen (H), oxygen (O), sulfur (S), nitrogen (N) 2. Possess primary, secondary, tertiary (sometimes quaternary) structure 3. Same properties as other proteins a. Charge (isoelectric point, electrophoresis) b. Solubility c. Denaturation (extremes in heat, pH, chemical) d. Non-specific or specific (antigenic) binding 4. Some enzymes have iosenzyme forms: a. Different form of an enzyme due to differing arrangements of the polypeptide units in the quaternary structure b. Maintains specificity for the same chemical reaction c. Possess unique diagnostic value: show specificity to certain organ systems 1) Isoenzymes of creatinekinase (CK) CK-MM to skeletal muscle CK-MB to cardiac tissue CK-BB 2) Isoenzymes of lactate dehydrogenase (LD) LD1 and LD2 to cardiac tissue LD4 and LD5 to liver and skeletal muscle
B. Biochemical Function 1. Catalyze chemical reactions: accelerates specific chemical reactions toward equilibrium S P Substrate (S) + Enzyme (ES Product (P) +Enzyme
2. Lowers the energy of activation required for the reaction to proceed
3. Properties of enzymes a. Effective in small concentrations b. Remain unchanged in the reaction, not consumed in the reaction c. Effect speed of reaction (not final concentration of substrate or products) d. Show greater degree of specificity than chemical catalysts e. Unstable and easily destroyed
4. Cofactors:substances associated with some enzymes that are needed formaximal enzyme activity • Coenzyme: organic cofactors (NAD, NADH); serve as second substrates for enzyme reactions b. Activators: inorganic cofactors (Ca++, Fe++, Zn++, K+, Mg++)
C. Importance of Enzymes in Health and Disease 1. Enzymes are intracellular 2. Enzyme concentration differs dependent upon type of tissue a. AST: high concentration in liver b. Amylase: high concentration in pancreas and salivary glands
Enzymes of Clinical Significance • CreatineKinase • 1. Specimen collection and handling • a. Serum is preferred, especially if fractionation/electrophoresis also • ordered • b. Heparinized plasma may be acceptable; • Many anticoagulants (fluoride, EDTA, sodium citrate) inhibit • enzyme activity and required activators (Ca2+, Mg2+) • c. No hemolysis: intracellular components interfere with chemical • reaction in laboratory measurements (NADH, ATP, HK, etc) • d. Avoid lipemia, especially for spectrophotometric analysis • e. Relatively unstable: analyze within 4 hours of collection, else • stable at 2-6oC for up to one week; stability increases when stored • at lower temps (-20oC)
Wide tissue distribution: injury, tissue necrosis will cause elevation of this enzyme in plasma/serum a. Skeletal muscle b. Heart tissue c. Brain, nerve tissue
Method of Measurment 3. Physiologic reaction: CK is a transferase: ATP storage and generation in contractile or transport systems, predominantly in muscle cells. Creatine + ATP CK creatinephosphate + ADP 4. Method of measurement Most common method: modified Rosalki-Oliver method creatine phosphate + ADP CK creatine+ ATP ATP + glucose HK ADP + glucose-6-phosphate Glucose-6-phosphate + NADP+ G6PD 6-phosphogluconate +NADPH (Increased ABS at 340 nm)
Isoenzymes: clinical relevance of CK activity often depends more on isoenzyme fractionation than on total levels: a. Isoenzymes occur as a dimer: 1) B polypeptide units 2) M polypeptide units b. Three isoenzyme forms: numbered by their anodal (+) electrophoresis mobility with ‘fraction 1’ migrating fastest towards the anode 1) CK1 = CK-BB (brain type) Normal: ~0% 2) CK2 = CK-MB (hybrid, heart) Normal: <5% 3) CK3 = CK-MM (muscle type) Normal: 95-100%
c. Immunologic measurement of CK-MB 1) Immunoinhibition of subunit M (anti-M) 2) Measure CK before and after inhibition 3) Disadvantage: falsely elevated if CK-BB activity present
d. Enzyme immunoassay measurement of CK-MB (mass) A ‘sandwich technique’ that uses 2 antibodies: one directed against the ‘M’ subunit, the other against the ‘B’ subunit which is also labeled with a reagent enzyme that catalyzes the conversion of substrate to product
6. Reference Ranges: affected by gender, • muscle mass, exercise, age • Total CK: • Male: 15-160 IU/L • Female: 15-130 IU/L • CK-MB: <5% of total CK
7. Clinical significance a. Acute Myocardial Infarction (AMI) 1) Increased total CK, increased CK-MB 2) Total CK increase 7-12 times normal with rise apparent at 4-6 hours post MI peaks at 18-24 hours and returns to normal by 72 hours 3) The rise, peak and fall of CK-MB parallels that of total CK, but a little sooner 4) Other cardiac events (trauma/inflammation) variable results
b. Skeletal muscle disease 1) Increased total CK, normal CK-MB (increased CK-MM) 2) Muscular dystrophy, especially Duchenne type: may see total CK 50x ULN 3) Inflammation of muscle, especially viral, also malignant hyperthermia 4) Normal CK activity in neurogenic muscle disorders: multiple sclerosis, myasthenia gravis, poliomyelitis
c. Central nervous system disorders 1) Increased total CK, normal CK-MB (increased CK-BB) 2) Trauma or pathology indicated when CK-BB is present 3) Cerebral vascular disease, encephalopathy, stroke (CK-BB )may be normal
d. Other 1) Neonates: normally have 1-3% CK-BB 2) Hypothyroidism: increased total CK, increased CK-MM 3) CK activity is NORMAL in liver disease 4) Effect of hemolysis is procedural and not due to CK activity in RBC
B. Lactate dehydrogenase (LD)1. Specimen collection and handling a. Serum is preferred, especially if fractionation/electrophoresis also ordered b. Heparinized plasma may be acceptable; many anticoagulants (fluoride, EDTA, sodium citrate) inhibit enzyme activity c. No hemolysis: LD-1 activity in the RBC is 150x greater than that in plasma d. Avoid lipemia, especially for spectrophotometric analysis e. Relatively unstable: analyze within 4 hours of collection, else stable at 2-6oC for up to one week; stability increases when stored at lower temps (-20oC) f. LD-4 and LD-5 are especially labile: stable when stored at room temperature, do not store in refrigerator or freezer unless glutathione is added as preservative
2. Wide cellular/tissue distribution a. Skeletal muscle b. Cardiac muscle/tissue c. Liver d. RBC e. Kidney, lung, tumor cells
3. Physiologic reaction: • LD is an oxidoreductase: catalyzes the • interconversion of lactic and pyruvic acids • Lactate + NAD+ LD Pyruvate+ NADH + H+
4. Method of measurement Forward reaction: Lactate + NAD+ ---LD (pH 8.3-8.9)Pyruvate + NADH +H+ (Increased ABS at 340 nm) Reverse reaction: Pyruvate + NADH ---LD (pH 7.1-7.4) Lactate + NAD+ (Decreased ABS at 340 nm)
Both the forward and reverse reactions have been used in the clinical lab, with the rate of the reverse reaction being ~3 times faster allowing measurement of smaller sample volumes and shorter reaction times. However, the forward reaction has better linearity at this time
5. Isoenzymes: clinical relevance of total LD activity often depends more on isoenzyme fractionation correlating to total LD activity a. Isoenzymes occur as a tetramer 1) H polypeptide units (heart) 2) M polypeptide units (muscle)
b. Five isoenzyme forms: numbered by their anodal electrophoresis 6. Reference Ranges: Total LD 100-200 IU/L LD-1 14-26% of total LD LD-2 29-39% of total LD LD-3 20-26% of total LD LD-4 8-16% of total LD LD-5 6-16% of total LD
mobility with ‘fraction 1’ migrating fastest towards the anode (+) 1) LD1 = HHHH Heart, RBC, kidney 2) LD2 = HHHM 3) LD3 = HHMM 4) LD4 = HMMM Skeletal muscle, liver 5) LD5 = MMMM 6. Reference Ranges: Total LD 100-200 IU/L LD-1 14-26% of total LD LD-2 29-39% of total LD LD-3 20-26% of total LD LD-4 8-16% of total LD LD-5 6-16% of total LD
7. Clinical significance: a. Hepatocellular disease 1) Increased total LD (7-10 x ULN), increased LD-4, LD-5 2) Toxic and viral hepatitis; infectious mononucleosis 3) Normal or slightly elevated in obstructive liver disorders b. Skeletal muscle disease 1) Increased total LD, increased LD-4 and LD-5 2) Muscular dystrophy, especially Duchenne type Skeletal muscle, liver
c. Acute myocardial infarction (AMI) • Increased total LD, increased LD-1 and LD-2 with a flipped ratio 2) Total LD increases 3-7 times normal with rise apparent at 8-12 hours post MI peaks around 72 hours and returns to normal by 7-12 days 3) Not useful for diagnosis of AMI 4) Other cardiac events (trauma/inflammation) variable results
d. Hemolytic anemia 1) Increased total LD 20-50 times normal, increased LD-1 and LD-2 with a false flipped ratio (not due to MI) 2) Untreated Pernicious Anemia, FolateMagaloblastic Anemia 3) Hemolytic anemia
C. AspartateTransaminase (AST) Historical:Serum glutamate oxaloacetatetransaminase (SGOT) 1. Specimen collection and handling a. Serum preferred, heparinized plasma acceptable; other anticoagulants inhibit enzyme activity b. Avoid hemolysis: RBC contain AST c. Avoid lipemia, especially for spectrophotometric analysis d. Relatively stable: analyze within 8 hours of collection, else store at 2-4oC for up to 4 days
2. Wide cellular/tissue distribution • Skeletal muscle b. Cardiac muscle/tissue c. Liver d. Kidney, pancreas, RBC
3. Physiologic reaction: AST is a transferase; catalyzes the transfer of an amino group between aspartate and alpha-keto acids. Important in the synthesis and degradation of amino acids; ketoacids formed are used in the TCA cycle to provide a source of energy Aspartate + α-ketoglutarate AST Oxaloacetate+ Glutamate
4. Method of measurement: Karmen method Aspartate + alpha-ketoglutarate AST Oxaloacetate + Glutamate Oxaloacetate + NADH + H+ Malate + NAD+ (decreased ABS at 340 nm)
5. Reference Range: 0-56 IU/L • a. Liver disease: hepatocellular, parenchymal disease • 1) Inflammation: toxic or viral hepatitis, infectious • mononucleosis; activity may reach up to 50-100 x normal • 2) Obstructive conditions (cholestasis, some stages of • cirrhosis) generally show normal or slightly increased AST
6. Clinical significance • a. Liver disease: hepatocellular, parenchymal disease • 1) Inflammation: toxic or viral hepatitis, infectious • mononucleosis; activity may reach up to 50-100 x normal • 2) Obstructive conditions (cholestasis, some stages of • cirrhosis) generally show normal or slightly increased AST
b. Skeletal muscle disease 1) Muscular dystrophy, especially Duchenne type 2) Inflammation of the muscle, malignant hyperthermia, crushing muscle injury 3) Neurogenic muscle disorders such as multiple sclerosis, myasthenia gravis, poliomyelitis show normal AST