Download
1 / 62
640 likes | 1k Views
APRN Practice in Texas. Kathy Shipp MSN, APRN, FNP . Disclosures. President, Texas Board of Nursing (BON) Presentation was prepared with the assistance of BON staff

E N D
APRN Practice in Texas Kathy Shipp MSN, APRN, FNP
Disclosures President, Texas Board of Nursing (BON) Presentation was prepared with the assistance of BON staff It is the policy of the BON to ensure balance, independence, objectivity and scientific rigor in all of its continuing nursing education activities No conflicts of interest to disclose Discussions today do not imply endorsement of any commercial product or off-label use of any product for which it was approved by the FDA
Objectives • Discuss the Nursing Practice Act (NPA) and BON Rules and Regulations as they apply to advanced practice registered nurses (APRNs) • Differentiate the roles and function of the BON from those of nursing and healthcare specialty associations
Objectives Discuss the 83rd Legislative Session, new legislation and Continuing Competency Requirements Discuss New BON Rules and Regulations Discuss physician delegation of prescriptive authority and SB406
Board of NursingAgency Mission To protect and promote the welfare of the people of Texas by ensuring that each person holding a license as a nurse in the State of Texas is competent to practice safely
Role of the Board Regulation of Nursing Practice Approval of nursing education programs Licensing qualified applicants Investigating complaints Corrective Action / Discipline
Texas (December 2013) APRN • 98,056 LVNs (26%) • 260,717 RNs (69%) • 17,597 APRNs (5%) Total 376,370 LVN RN
Board of Nursing • Responsible to the public • No authority in employment related issues, i.e. facility policies and procedures • Prohibited by law from lobbying legislature • Organizations & Associations • Responsible to their members • Serve the individual interests of nurses • May lobby legislature and Governor
Board Members • 13 members • Nursing Education 1 – LVN education 1 – ADN education 1 – BSN education • Consumers - 4 • Representing: Nursing Practice 3 – LVN in active practice 2 – RN in active practice 1 – Advanced Practice RN (APRN) in active practice
Board Meetings • Quarterly meetings (January, April, July, & October) • Dates posted on website and Bulletin • Meetings open to the public • Held in the Hobby Building in Austin • Receive input from stakeholders
Advisory Committee • Advisory Committee on Education (ACE) • Nursing Practice Advisory Committee (NPAC) • Advanced Practice Advisory Committee (APAC) • Eligibility and Disciplinary Advisory Committee (EDAC) • Task Force – Delegation Task Force (DTF)
Our Practice Staff Kristin Benton, MSN, RN, Director of Nursing Jackie Ballesteros Denise Benbow, MSN, RN Nicole Binkley, BSN, RNC Bonnie Cone, MSN, RN Melinda Hester, DNP, RN Laura Lewis Ciara Williamson Jolene Zych, PhD, RN, WHNP-BC
Nursing Licensure Compact • Multistate license privilege • Legal agreement between states • Texas is a Compact State • A party state can rescind the nurse’s multistate licensure privilege and report violations to nurse’s home state • Home state can take action • APRNs do not have a compact at this time NPA, Chapter 304 Board Rules Chapter 220
Continuing Competency Requirements NEW LEGISLATION 83rd Legislative Session • SB 1058 (Effective September 1, 2013) • 2 Hours of CE in adults/geriatrics for those whose practice includes adult and geriatric populations each renewal cycle • 2 Hours of CE in Nursing Jurisprudence and Ethics each third renewal (every 6 years) • SB 1191 (Effective September 1, 2013) • 2 hours of CE in forensic evidence collection for any nurse who performs a forensic examination on a sexual assault survivor (Not just Emergency Department nurses)
83rd Legislative Session • SB 1058 (Effective September 1, 2013) • In addition to targeted CNE - Mandatory criminal background checks for students • SB 945 (Effective January 1, 2014) • Requires a health care provider in a hospital to wear a photo identification badge clearly stating the provider's name, department, title, type of license held. • If applicable, the badge must also state the provider's status as a student, faculty, intern, trainee, or resident.
83rd Legislative Session • SB 1842 (Effective Immediately – June 14, 2013) • In hospitals and state mental hospitals, patients will have a face to face assessment within one hour after initiation of a restraint or seclusion by a RN who has special training and did not initiate the restraint or seclusion. • HB 705 (Effective September 1, 2013) • Enhances penalty prescribed for an assault committed against emergency services personnel.
83rd Legislative Session • SB 406 (Effective November 1, 2013) • Made changes to delegative authority in the State of Texas. • FAQs on the website • New Rule Chapter 222 • For additional information go the Website; and /or contact the APRN Department (aprn@bon.texas.gov)
UPDATE: • New Board of Nursing Rules and Regulations • Proposed • Adopted by Board at Quarterly Meeting • Jan 2014 : Chapter 216 – continuing competency • Jan 2014 : Chapter 228 – Pain Management – minimum standards of nursing practice for APRNs when providing pain management services
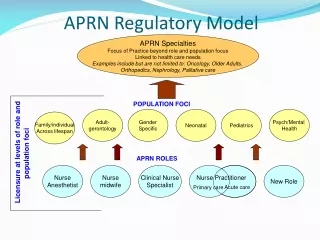
APRN Continuing Competency Requirements For APRN licensure renewal: 20 contact hours of targeted continuing education in the advanced practice role and population focus area recognized by the BON or attain, maintain, or renew the national certification recognized by the BON
APRN Continuing Competency Requirements • For Prescriptive Authority Renewal: +5 additional CEs in Pharmacotherapeutics within the preceding 2 years +3 additional hours related to prescribing controlled substances for those who prescribe controlled substances The 20 CEs satisfy both the RN and APRN requirement Category I Continuing Medical Education (CME) contact hours will meet requirements for CE for APRNs
Prescriptive Authority (Rx Auth) • APRN Licensure AND prescriptive authority • Texas Medical Board Delegation of Prescriptive Authority (www.tmb.state.tx.us) • Texas Department of Public Safety (DPS) AND US DEA controlled substances registration
Dangerous Drugs • Texas Health and Safety Code, § 483 • Legend drugs • “Caution: federal law prohibits dispensing without prescription” • “Rx only” • Does not require DPS and DEA numbers
Controlled Substances • Code of Federal Regulations § 1308 • Texas Health and Safety Code § 481 • Defines each schedule
Controlled Substances • Schedules III through V in any setting • Schedule II • Certified terminally ill patients with qualified hospice provider • Hospital facility based practicein hospital emergency departments • Hospital facility based practice for hospitalized patients intended to stay at least 24 hours
Controlled Substances • No more than 90 day supply • Collaboration and documentation for refills and for prescriptions for children less than two years • DPS and DEA registrations required
Additional Clarifications • Nonprescription drugs • Durable medical equipment (DME) • Order or prescribe in most cases • CRNAs not required to have prescriptive authority
Mechanisms for Delegation of Prescriptive Authority • Protocols or other written authorization • Facility based practices only • Prescriptive authority agreement
Prescriptive Authority Agreement An agreement entered into by a physician and an advanced practice registered nurse or physician assistant through which the physician delegates to the advanced practice registered nurse or physician assistant the act of prescribing or ordering a drug or device.
Before Executing A Prescriptive Authority Agreement • Current APRN license and prescriptive authority in good standing • Not prohibited by Board of Nursing • Disclosure of any prior discipline
What Has to Be Included? • Signed and dated by the parties to the agreement & reviewed/resigned at least annually; • Name, address, and all professional license numbers of the parties to the agreement; • State the nature of the practice, practice locations, or practice settings; • Identify the types or categories of drugs or devices that may be prescribed OR the types or categories of drugs or devices that may not be prescribed;
Requirements for Prescriptive Authority Agreement • Provide a general plan for addressing consultation and referral; • Provide a plan for addressing patient emergencies; • State the general process for communication and the sharing of information between the physician and the APRN or PA to whom the physician has delegated prescriptive authority related to the care and treatment of patients; • Designate one or more alternate physicians
Quality Assurance & Improvement Plan Document a quality assurance and improvement plan and specify methods for implementation of the plan to include: • Chart review • Periodic face to face meetings
Face to Face Meetings • At least monthly until the 3rd anniversary of the date the agreement is executed; • At least quarterly after the 3rd anniversary of the date the agreement is executed, with monthly meetings held between the quarterly meetings by means of a remote electronic communications system, including videoconferencing technology or Internet;
Face to Face Meetings During the 7 years preceding the date the agreement is executed the APRN or PA for at least 5 years was in a practice that included the exercise of prescriptive authority with required physician supervision: • At least monthly until the 1st anniversary of the date the agreement is executed; and • At least quarterly after the 1st anniversary of the date the agreement is executed, with monthly meetings held between the quarterly meetings by means of a remote electronic communications system, including videoconferencing technology or the Internet
Credit for Rx Authority Experience The calculation under Chapter 157, Texas Occupations Code, of the amount of time an APRN or PA has practiced under the delegated prescriptive authority of a physician under a prescriptive authority agreement shall include the amount of time the APRN or PA practiced under the delegated prescriptive authority of that same physician prior to November 1, 2013. You must be practicing with the same physician you practiced with prior to November 1, 2013 in order to get credit under this provision.
Additional Content • Other mutually agreed upon provisions • Need not describe exact steps • Promote exercise of professional judgment • Keep copy of agreement for 2 years • Cannot nullify, void or waive requirements by contract
APRN to Physician Ratio • In many cases: • 1 Physician • 7 Full time equivalent APRNs/PAs • No limits in facility-based practices in hospitals or practices serving a medically underserved population
Investigations & Discipline • Notify other parties to agreement if investigation is opened • Make agreement available to the board(s) not later than the 3rd business day after receipt of a request • Boards of nursing, medicine and physician assistants notify each other if investigation opened involving prescriptive authority and final disposition. • Open investigation based on notice from other boards • Publish list of APRNs prohibited from entering prescriptive authority agreement • Texas Medical Board onsite inspection authority
FAQs on BON Websiteand TMB Website Also provided to you as a handout.
Board Rules Applied to APRNs Rule 217.11 Standards of Nursing Practice Rule 217.12 Unprofessional Conduct Rule 221.13 Core Standards for Advanced Practice Rule 222.4 Minimum Standards for Signing Prescriptions
Rule 217.11 • Four subsections: • (1) applies to all nurses at all levels of licensure • (2) applies to LVNs • (3) applies to RNs • (4) applies to APRNs • Subsections (1), (3) and (4) are applicable to APRNs
(1)(B) Implement measures to promote a safe environment
(1)(C) Know the rationale for and effects of medications and treatments and shall correctly administer the same For APRNs, this also means knowing the rationale for and effects of medications and treatments that are ordered or prescribed.
Rights of Medication Administration • Patient • Medication • Dose • Route • Time • Documentation • Reason/Diagnosis • Assessment • Patient education • Patient response • Refuse medication
(1)(T) Accept only those nursing assignments that take into consideration client safety and that are commensurate with the nurse’s educational preparation, experience, knowledge, and physical and emotional ability.
217.11(3) and (4) Rule 217.11(3) includes standards related to a systematic approach to patient care and addresses delegation to unlicensed personnel Rule 217.11(4) requires APRNs to practice and prescribe in accordance with the role and population focus of licensure
217.12 Unprofessional Conduct Applies to all nurses Describes unprofessional or dishonorable behaviors Public protection
217.12(1)(A) and (4) • 217.12(1)(A) • Carelessly failing, repeatedly failing, or exhibiting an inability to perform vocational, registered or advanced practice nursing in conformity with the standards of minimum acceptable level of nursing practice. . . . • 217.12(4) • Careless or repetitive conduct that may endanger a client’s life, health or safety. Actual injury to a client need not be established.
Other Behaviors Include: Failure to supervise students appropriately Failure to practice within a modified scope Inability to practice safely Misconduct—falsification, abuse, boundary violations, threatening behavior Criminal conduct