Download
1 / 38
500 likes | 1.52k Views
Tubular reabsorption & Secretion. Dr. Eman El Eter. Juxtamedullary nephrons vs Cortical nephrons. Urine Formation Preview. Introduction. Urinary excretion = Glomerular Filtration –Tubular reabsorption + Tubular secretion. Tubular secretion means:

E N D
Tubular reabsorption & Secretion Dr. Eman El Eter
Introduction • Urinary excretion = Glomerular Filtration –Tubular reabsorption + Tubular secretion. Tubular secretion means: the net movement of solutes from peritubular capillaries into the tubules.
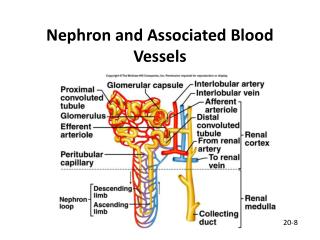
What are the routes through which a substance enter the tubules? 1- Glomerular filtration. 2- Secretion from the peritubular capillaries which occurs in two steps: a. simple diffusion of the substance from peritubular capillaries into renal inerstitium. b. movement across the tubular epithelium into the lumen through active or passive transport.
Mechanisms of tubular transport: • Active transport: • Primary active transport: e.g. Na-K-pump, H+-pump • Secondary active transport : e.g. Na-K-2Cl co-transport, glucose-sodium co-transport, amino acid-sodium co-transport. • Passive transport: • Simple diffusion e.g. Cl, HCO3-, urea. • Facilitated diffusion glucose at the basal border. • Osmosis. • Thus the molecules moves through ion channels, transporters, pumps & exchangers. • Pinocytosis/ exocytosis.
Renal tubular reabsorption through PCT • Solute reaborption in the proximal tubule is isosmotic (water follows solute somatically and tubular fluid osmolality remains similar to that of plasma= equal amount of solute and water are reabsorbed). • 65%-70% of water and sodiumreabsorption occurs in the proximal tubule • 90% of bicarbonate, calcium, K+ • 100% of glucose & amino acids • Proximal tubules: coarse adjustment. • Distal tubules: fine adjustment (hormonal control).
Loop of Henle • Responsible for producing a concentrated urine by forming a concentration gradient within the medulla of kidney. • When ADH is present, water is reabsorbed and urine is concentrated. • Counter-current multiplier.
Absorption through loop of Henle: • Descending limb: is water permeable and allow absorption of 25% of filtered H2O. It is impermeable to Na-CL. • Thin ascending limb: is impermeable to H2O, but permeable to Na-Cl, where they are absorbed passively in this part . • Thick ascending limb: is impermeable to H2O. Na-K-2Cl co-transport occur in this part. By the end of ascending limb of loop, the tubular fluid becomes hypo-osmolar to plasma.
Distal convoluted tubule and collecting ducts • What happens here depends on hormonal control: • Aldosterone affects Na+ and K+ • ADH – facultative water reabsorption • Parathyroid hormone – increases Ca++ reabsorption. • Fine adjustment of tubular filtrate takes place here according to body needs. • The first portion of DCT forms part of JGA, that provides feedback control of GFR and RBF of the same nephron. • The next early portion has the same characteristics as ascending limb of Henele that is impermeable to water but absorbs solutes. So it is called the diluting segment & the osmotic pressure of the fluid ~ 100 mOsm/L.
Late distal tubule& collecting tubules • Have similar functional characteristics. • Composed of two types of cells: • a. Principal cells: absorb Na+& H2O and secrete K+ • b. Intercalated cells: absorb K+ & secrete H+ • Impermeable to Urea. • water permeability under ADH • Secretion of K+ and reabsorption of Na+ controlled by aldosterone.
Medullary collecting ducts • Reabsorb <10% of sodium & H2O. • Final site for processing urine and so determine final urine output of H2O & solutes • Characteristics: - Under ADH control. -Highly permeable to urea. -Secretes H+ against conc gradient (role in acid-base balance).
Na+, K+, H+ urea
Distal convoluted tubule and collecting ducts • Tubular secretion to get rid of substances: K+, H+, urea, ammonia, creatinine and certain drugs • Secretion of H+ helps maintain blood pH (can also reabsorb bicarb and generate new bicarb)
Na+ absorption • Na & Cl reabsorption plays a major role in body electrolyte and water metabolism. • Na+ transport is also coupled to the movement of H+, K+, glucose, amino acids. • Na+ absorption occurs by many mechanisms depending on the part of nephron: • 1- active transport mechanism: • E.g. Collecting tubules & ducts. • 2- Passive at the thin ascending limb • 3- Co-transport: thick ascending • i.e. Active all through except thin ascending limb.
From tubular lumen into tubular cells Na+ moves by; Exchanger Co-transport. It helps reabsorption of nutrients Na+ is pumped into the interstitium by Na+-K+ ATPAse
Glucose handling • Glucose absorption also relies upon the Na+ gradient. It is absorbed by Na-glucose co-transport. • Most reabsorbed in proximal tubule. • At apical membrane, needs Na+/glucose cotransporter (SGLT) • Crosses basolateral membrane via glucose transporters (GLUT’s), which do not rely upon Na+.
Tubular transport maximum for glucose • Essentially all glucose is reabsorbed • Tmg = 375 mg/min in men and 300 mg/min in women. • The renal threshold for glucose= 180 mg/dl • Handling of glucose is limited by saturation of the transport mechanism i.e. carriers.
Glucose titration curve • Ideal curve occurs if Tmg in all tubules is identical and if glucose was removed from all tubules . • Actual curve is rounded (dashed line) and deviates from the ideal curve. This deviation is called splay. • The magnitude of the splay is inversely proportionate to the avidity with which the transport mechanism binds the substance it transports.
Water reabsorption • PCT: 65% of filtered water reabsorbed. • Descending loop of Henle:20-25% . • Ascending limb= zero water reabsorbed.
Regulation of tubular reabsorption • There must be a balance between tubular reapsorption and glomerular filtration. • This is controlled by local , nervous & hormonal mechanisms. • Do you think that water and solutes are dependently regulated? • 1.Glomerulotubular balance; prevents overloading of distal parts when GFR increases. • 2. Peritubular capillary reabsorption is regulated by hydrostatic and colloidal pressures through the capillaries. • 3. ABP: if increased it reduces tubular reapsorption.
Regulation of tubular reabsorption, cont…… • 4-Tubuloglomerular feedback: • What is its physiological importance?
Regulation of tubular reabsorption, cont…… • 4. Hormonal: • - Aldosterone: Na+ Reabsorption, K+&H+ secretion • -Ang II.: (+)Aldosterone • ADH (+) H2O2 reabsorption • ANP: (+)Na+ excretion & diuresis • Parathyroid hormone: Increases calcium reabsorption & decreases phosphate reabsorption. • Nervous: Sympathetic: -Increases Na+ reabsorption.
K+ handling • K+ is the major cation in cells and its balance is essential for life. • Small change from 4 to 5.5 mmoles/l = hyperkalaemia • K+ is reabsorbed at proximal tubule. • Changes in K+ excretion due to changes in K+secretion in distal tubule
K+ handling • K+reabsorption along the proximal tubule is largely passive and follows the movement of Na+ and fluid. • K+secretion occurs in cortical collecting tubule (principal cells), and relies upon active transport across basolateral membrane and passive exit across apical membrane into tubular fluid.