Download
1 / 34
340 likes | 417 Views
Simulating Diffusion Processes on Very Large Complex networks. Jiangzhuo Chen. Joint work with Keith Bisset, Xizhou Feng, Madhav Marathe, and Anil Vullikanti. SIAM Conference on Parallel Processing for Scientific Computing (PP10) February 25, 2010. Talk Outline.

E N D
Simulating Diffusion Processes on Very Large Complex networks Jiangzhuo Chen Joint work with Keith Bisset, Xizhou Feng, Madhav Marathe, and Anil Vullikanti SIAM Conference on Parallel Processing for Scientific Computing (PP10) February 25, 2010 Network Dynamics & Simulation Science Laboratory
Talk Outline • Background: simulation of infectious disease propagation on social contact networks • HPC-based parallel epidemic simulation tools developed at NDSSL: • EpiSims • EpiSimdemics • EpiFast • Indemics • Summarize
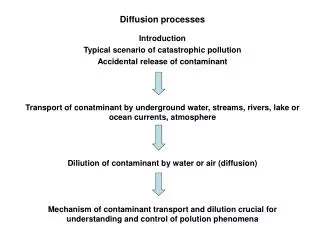
Epidemic Simulation • This talk will focus on simulating a major diffusion process – epidemic evolution – on large scale social contact networks • Models and ideas can be extended to other diffusion processes on large scale networks like: • Norms and fads in social networks • Worms in communication networks
Disease Spread in a Social Network • Within-host disease progression is modeled as a local state transition function, called PTTS (probabilistic timed transition system) • Health states include: susceptible, infected but not infectious (incubating), infectious but asymptomatic, infectious and symptomatic, recovered. • State transitions are probabilistic and timed • Between-host disease transmission occurs along edges of a social contact network • Represented by people-location graph or people-people graph • Transmissions are probabilistic • Probability of a person getting infected depends only on his local properties and people that he has contact with: symmetry assumption
Interventions • Pharmaceutical interventions (PI’s): vaccination or antiviral changes an individual’s role in the transmission chain • Lower susceptibility to infection • Lower infectiousness if infected • The degree these are lowered depends on the efficacy of the vaccine or antiviral • Non-pharmaceutical interventions (NPI’s): social distancing measures change people activities and change the social network • Generic social distancing, school closure, isolation, etc. • Interventions are often associated with trigger conditions and selected subpopulations • When, how, and to whom these are applied can have different impact on the course of the epidemic
EpiSims: Precise Simulation • Parallel discrete event simulation (PDES) • Within-host disease progression: coupled PTTS (probabilistic timed transistion system) • Between-host disease transmission: people-location bipartite graph • Complex interventions: • NPI’s change people activity schedules, so change people-location graph • PI’s change people susceptibility/infectivity
EpiSims: Parallel Algorithm • Symmetric computations among processors • Locations are partitioned and assigned to processors • Each person v has corresponding data Dv(demographics, health state, activity schedule, etc.) • Dvis moved from the processor which has location A to the processor which has location B if v moves from A to B • System synchronizes at every event: person changes activity location, person health state changes, etc.
EpiSims: Performance • Too many events: too many synchronizations • High communication cost for moving data between processors • Scales poorly for large urban populations (size > 10 million) • Simulation running time: magnitude of hours~days for Chicago (9 million people) • Good for small populations or small number of replicates
EpiSimdemics: Fast Simulation • Parallel discrete time simulation • Within-host disease progression: coupled PTTS (highly configurable disease model) • Between-host disease transmission: people-location bipartite graph • Complex interventions specified by scenario scripting language: • NPI’s change people activity schedules, so change people-location graph • PI’s change people susceptibility/infectivity
EpiSimdemics: Peformance • Parallel algorithm: • Partition locations and assign them to processors • Partition people and assign them to processors • At each time step, for each location compute a serial DES; system synchronization • Approximations (from PDES): • discrete time simulation • Relaxation of causality constraint: system synchronization at every time step (every simulation day) • C++/MPI implementation • Scaling: 100 million people on 1k cores • Simulation running time: magnitude of hours for large urban populations
EpiSimdemics Algorithm Generate the population Set initial infections Based on activities move the people to the locations Compute interactions among the people at the locations Some exposed people may become infected After their activities, the people are moved back to their home PE Update state of person at his home PE
EpiSimdemics: Use Case • Flu in Alabama • Similar to studies done for sponsors (NIH, CDC, DTRA, etc.) • Population size = 4.3 million • 4 interventions (16 combinations) • Vaccination (prevaccinate children, critical workers) • School closure (close/reopen on per county basis) • Quarantine of critical workers • Self isolation (when global attack rate is high)
Results for Critical Workers • Quarantine of critical workers has no effect on the general population • When critical workers are vaccinated and quarantined, their infection rate drops from 40% to 18% • May be important for continuous functioning of society
EpiFast: Faster Simulation Parallel discrete time simulation based on percolation model Within-host disease progression: standard SEIR disease model Between-host disease transmission: through edges of people-people contact network Interventions Pharmaceutical or non-pharmaceutical: predefined impacts on network nodes and edges On day <t> or when a given threshold <x> is met, apply intervention <i> on subpopulation <s>
EpiFast: Social Contact Network • From people-location graph to people-people contact network: • People follow daily activity schedules • Activities take them to locations • At locations they interact with each other • Interactions form contact network • Nodes are people, edges are contacts, edge weights are contact durations • Interactions in a population can get very complex • e.g. New York city has 18 million people and a total of 1 billion interactions • Disease spread in contact network depends on • Duration of contact • Types of activities while in contact • Characteristics of the infectious person • Characteristics of the susceptible person • EpiFast assumes the network remains the same from day to day unless with interventions
EpiFast: Algorithm Parallel implementation: Master-slave model Partition contact network: each slave processor is assigned a subset of nodes and all outgoing edges Single master processor: communication; many slave processors: computation Highly portable C++/MPI implementation Approximations (from PDES): Network edges (contacts) are not ordered by time Network remains the same from day to day unless with interventions Synchronizes every simulation day Interventions change the contact network (node or edge properties); changes are approximate
EpiFast: Performance By far the fastest (to our best knowledge) among all epidemic simulations that can handle realistic synthetic populations and provide comparable support for realistic intervention measures. Network of 16 million nodes and 900 million edges: <20 minutes per replicate on as few as 32 processors Scales well on distributed memory systems Good strong and weak scaling properties
EpiFast: Use Case Factorial design: 2x2x2x2 x 25 replicates = 400 runs
Indemics: Interactive Simulation • Indemics: Interactive EpidemicSimulation and Modeling Environment • New data-centric architecture for interactive epidemic simulation environments • Decouples the data, disease diffusion, intervention and user interaction • Simplify design and implementation of simulation engine • performance can be optimized separately • High performance computing service architecture • User can access the system via a web server from anywhere • HPC-based system supports coordination, data management and disease diffusion • Reduction in speed is easily compensated by ease of interaction and rich feature set
Indemics: System Architecture Indemics database running on a data server Indemics Server, running on head node of HPC Indemics Server Semi-structured database Temporal database Relational database New Interventions Queries & Interventions New disease state Indemics Adapter Indemics Adapater Interactive Client Batch Client HPC Epidemic Simulator (e.g. EpiFast) Indemics web-interface Client,on PC Analyst sees only this module
Indemics: Abstractions • Data Models: • Relational data about individuals (P) • Social contact network (N) • Transmission network/dendrogram (D) • Models of Interaction between user, data and model • Query: function of (P,N,D) • E.g. who are sick, how many of a concerned subpop are sick • Does not change the disease progression • Can be expressed by SQL script • Intervention: active interaction • makes a change to the social network, individual behavior, or disease model; and moves the simulation forward • apply intervention <i> to subpopulation <g> with parameter <p>
Indemics: Queries • Queries on a single data type • (P) Find all school-age people in Seattle • (N) Find all network neighbors (contacts) of a specific person • (D) Find all people infected in last week • Queries across multiple data types • Count number of infected persons in zip code 24060 (Blacksburg, VA) • Find infectious students in Blacksburg high school and their family members • Users interact with the system using well-defined languages • Indemics commands: count infected persons : group = seniors, infected day = between 20 and 22 • SQL statements: select edge_head from network table SN and infection table INF where SN.edge_tail = INF.infected_pid and infection_day = 20 (find contacts of people infected on day 20) • Libraries of queries can be pre-defined by expert users
Indemics: Interventions • Intervention abstraction apply intervention <i> to subpopulation <g> with parameter <p> • Intervention types vaccination, antiviral, school closure, work closure, generic social distancing, etc. • Subpopulations (to which interventions are applied) • Predefined groups: preschool, school age, adult, senior, critical workers, etc • Dynamic group: result of any query e.g.: group g = {family members of persons who were infected on day 10} • Indemics command • apply interventions: type = antivirus, duration = 20, group = school age, infected_day = between 24 and 30 • apply interventions: type=work closure, duration = 20, group = adults, infected day = between 20 and 21; type = school closure, duration = 5, group = school age
Indemics: Performance • Simulates what the original simulator can simulate, with small overhead • E.g. same scenario: vaccinate preschools on threshold condition. Indemics occurs 70% overhead running time on top of EpiFast. • Far larger modeling capabilities with reasonably good performance • E.g. household level interventions were not supported in EpiFast. • Indemics can handle them easily. Cost of interaction and data communication is marginal (~20%) comparing with simulation cost. • Overhead for interactions is easily offset by infinitely larger capability and flexibility provided by Indemics.
Indemics: Use Case Public intervention versus private intervention: • Ring vaccination • Administered by public health authorities • All direct contacts of any infectious individual are identified and vaccinated (by government) • D1 vaccination • Individual self-motivated • People voluntarily take vaccines when they find the number of infectious people among their direct contacts exceed some threshold
Summary of Our Epidemic Simulation Tools • EpiSims: precise but slow; good for smaller populations and complicated scenarios and interventions. • EpiSimdemics: fast, good scaling; good for large populations and complicated scenarios and interventions but only a few replicates • EpiFast: fastest, good scaling; good for large population with simple scenarios and predefined interventions but large number of replicates • Indemics: most capable and flexible, extra running time; good for exploring various intervention strategies
Work funded in part by NIGMS, NIH MIDAS program, CDC, Center of Excellence in Medical Informatics, DTRA CNIMS, NSF, NeTs, NECO and OCI program, VT Foundation.