Download
1 / 23
320 likes | 801 Views
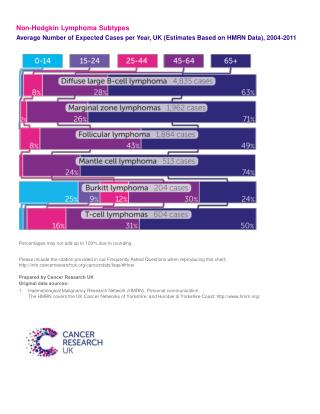
New aspects in the treatment of Hodgkin Lymphoma. Professor Andreas Engert on behalf of the GHSG. Treatment of Hodgkin Lymphoma. Background First-line treatment Treatment of relapse Summary. Prognosis of patients with Hodgkin Lymphoma by decades (the Vancouver experience).

E N D
New aspects in the treatment of Hodgkin Lymphoma Professor Andreas Engert on behalf of the GHSG
Treatment of Hodgkin Lymphoma • Background • First-line treatment • Treatment of relapse • Summary
Prognosis of patients with Hodgkin Lymphoma by decades (the Vancouver experience) 1.0 1990 .9 1980 .8 Cum Survival 1970 .7 .6 .5 1960 .4 .3 .2 .1 0.0 0 100 200 300 400 500 Disease specific survival (n=2075) Connors et al
Hodgkin Lymphoma: Clinical PresentationPatient R.M., 32 years
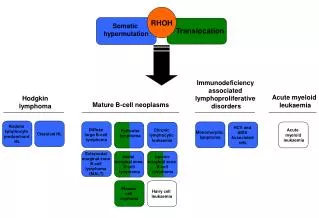
WHO Classification for HL (2001) Classical HL (cHL) • Lymphocyte-rich classical HL (5%) Nodular Sclerosis (60-80%) Mixed Cellularity (25-30%) Lymphocyte Depletion (1%) Nodular Lymphocyte predominant HL (5%)
GHSG clinical trials Recruitment of HL patients since 1978 1978 - 88 HD 1 - 3 506 1988 - 94 HD 4 - 6 2035 1994 - 98 HD 7 - 9 2865 1998 - 02 HD10-12 3948 2003 - 2/07 HD13-15 3717 Total 13071
Treatment of Hodgkin Lymphoma • Background • First-line treatment • Treatment of relapse • Summary
GHSG Risk groups Early favorable stages: CS I/II without risk factors* Early unfavorable stages: CS I/II with risk factors* Advanced stages: CS III/IV; selected CS IIB *a) large mediastinal mass; b) extranodal disease; c) high ERS; d) 3 or more areas
GHSG HD7 trial for early favorable HL CS/PS I, II without RF ABVD ABVD 30 Gy EF + 10 Gy IF Engert et al, JCO accepted
1.0 0.9 0.8 0.7 0.6 probability 0.5 0.4 EF: 67% at 7 years 2xABVD+EF: 88% at 7 years p<0.0001 0.3 0.2 0.1 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 years 2xABVD+RT RT GHSG HD7 trial for early favorable HL FFTF Engert et al, JCO accepted
HD10 trial for patients with early-favourable HL Design CS I/II without risk factors* 4 x ABVD 4 x ABVD 2 x ABVD 2 x ABVD 30 Gy IF 20 Gy IF 30 Gy IF 20 Gy IF *Large mediastinal mass; extranodal disease; high ERS; 3 or more areas involved GHSG 2001
1.0 0.9 0.8 0.7 0.6 Probability 0.5 0.4 0.3 p = 0.962 0.2 0.1 4ABVD 2ABVD 0.0 0 12 24 36 48 60 72 84 FFTF [months] Pts. at Risk 2ABVD 553 507 427 289 175 70 20 4ABVD 554 522 433 277 172 84 18 HD10 trial for patients with early-favourable HLFFTF by chemotherapy Survival curves are Kaplan-Meier estimations. Median follow-up time is 41 months, N=1107 Survival rates after 4 years of follow-up: 4xABVD: 94%; 2xABVD: 93%
1.0 0.9 0.8 0.7 Probability 0.6 0.5 0.4 0.3 p = 0.076 0.2 0.1 30Gy 20Gy 0.0 0 12 24 36 48 60 72 84 FFTF [months] Pts. at Risk 70 13 20Gy 537 506 420 272 169 30Gy 528 503 424 285 25 174 82 HD10 trial for patients with early-favourable HLFFTF by radiotherapy Survival curves are Kaplan-Meier Estimations, Median follow-up time is 41 months, N=1065 Survival rates after 4 years of follow-up: 30Gy: 94%; 20Gy: 93%
HD13 study for early favorable stages Design CS I/II without RF* ABVD ABVD ABV ABV AVD AVD AV AV 30 Gy IF 30 Gy IF 30 Gy IF 30 Gy IF *Large mediastinal mass; extranodal disease; high ERS; 3 or more areas involved
GHSG Risk groups Early favorable stages: CS I/II without risk factors* Early unfavorable stages: CS I/II with risk factors* Advanced stages: CS III/IV; selected CS IIB *a) large mediastinal mass; b) extranodal disease; c) high ERS; d) 3 or more areas
CS IA, IB, IIA with RF a-e CS IIB with RF d,e CS IIIA without RF a-e PS IIIA, N without RF a,c,d Randomisation Arm A 2 x (COPP/ABVD) Arm B 2 x (COPP/ABVD) Restaging 30 Gy EF + 10 Gy BULK 30 Gy IF + 10 Gy BULK HD8 trial for early unfavorable stages (1994-98; n=1136)
1.0 IF (30 Gy ) .8 .6 ) EF (30 Gy Probability .4 p = 0.543 .2 0.0 0 24 48 72 96 120 FFTF ( months ) GHSG HD8 Study for early unfavorable stages FFTF FFTF-rate [ 95%CI ] at 5 years: EF-RT (66 / 533): 85.9% [ 82 ; 89 ] IF-RT (72 / 533): 85.9% [ 83 ; 89 ] Engert et al JCO 2003
HD11 trial for patients with early unfavorable HL Design Stages I, IIA with RF a-d; IIB with RF c,d 4 x ABVD 4 x ABVD 4 x BEACOPP 4 x BEACOPP 30 Gy IF 20 Gy IF 30 Gy IF 20 Gy IF *a) large mediastinal mass; b) extranodal disease; c) high ERS; d) 3 or more areas
1.0 0.9 0.8 0.7 0.6 0.5 Probability 0.4 0.3 0.2 0.1 4xABVD 4xBEACOPP 0.0 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 Time [months] Pts. at Risk 4xABVD 649 584 453 301 259 168 78 4xBEACOPP 644 585 468 300 264 183 68 At 3 years 4xABVD: 87% 95% KI: [ 84 ; 90 ] 4xBEACOPP: 88% 95% KI: [ 85 ; 91 ] HD11 trial for early unfavorable HLFFTF by CT arm
1.0 0.9 0.8 0.7 0.6 Probability 0.5 0.4 0.3 0.2 0.1 30 Gy 20 Gy 0.0 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 Time [months] Pts. at Risk 296 261 177 76 30 Gy 634 591 467 20 Gy 636 578 454 305 262 174 70 At 3 years 30 Gy: 90% 95% KI: [ 87 ; 92 ] 20 Gy: 87% 95% KI: [ 84 ; 90 ] HD11 trial for early unfavorable HLFFTF by RT arm
30 Gy IF 30 Gy IF GHSG ongoing study for early unfavorable HL (HD14) Stages I, IIA with RF a-d; IIB with RF c,d ABVD ABVD ABVD ABVD BEACOPP escalated BEACOPP escalated ABVD ABVD *a) large mediastinal mass; b) extranodal disease; c) high ERS; d) 3 or more areas
Combined modality treatment for early HL Summary • 2xABVD equally effective to 4xABVD (HD10); radiotherapy question (20Gy or 30Gy) needs more follow-up • 2xABVD plus 30Gy IF new GHSG standard for early favorable • 4xBEACOPPbaseline more toxic than 4xABVD and equally effective in early unfavorable HL (HD11) • 4xABVD plus 30Gy IF remain GHSG standard for early unfavorable HL • Ongoing trials evaluate further reduction of toxicity for early favorable (HD13) and improving outcome for early unfavorable HL (HD14)