Download
1 / 90
900 likes | 1.15k Views
SNOMED Standards Development Organisation. College of American Pathologists National Health Service Connecting for Health. The SNOMED Standards Development Organization. Presentation 1: Content {suggested by CEN} What is this about? Why a terminology? Why SNOMED CT?

E N D
SNOMED Standards Development Organisation College of American Pathologists National Health Service Connecting for Health
The SNOMED StandardsDevelopment Organization • Presentation 1: Content {suggested by CEN} • What is this about? • Why a terminology? • Why SNOMED CT? • What will SNOMED NOT do? • Presentation 2: Organisation & Governance • What exactly is being proposed? • What are the finances? • What are the governance arrangements? • Why this arrangement MORE DETAIL ON CD & IN PACK
Presentation 1: Content • Special Thanks • Kevin Donnnelly and colleagues • Kent Spackman • Ian Arrowsmith • Mike Cooke • Grant Kelly
The SNOMED SDO: What is this about? • Data exchange / messaging • Terminology standards • Document standards • Information Model / EHR standards • Architecture standards • Application standards ABOUT ONE OF THE KEY STANDARDS TO SUPPORT INTEROPERABILITY OF EHR’S
The SNOMED SDO: What is this about? • An international effort to produce and enhance a global clinical terminology standard • An organization supporting that effort • A set of products and services produced
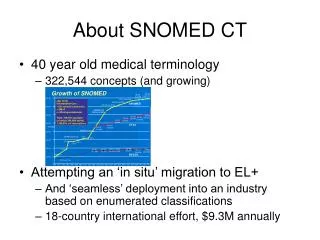
The SNOMED SDO: What is this about? • Scope of SNOMED CT UK Release [Core plus UK {local} extension] • Size (as of Jan 2005 UK Edition) • 414,808 health care concepts • 1,084,972 descriptions • 1,465,255 semantic relationships • English, German and Spanish language editions • Cross mappings (ICD-10, OPCS 4.2) • Extensions (UK Admin, UK Drugs)
FROM Proprietary [CAP] owned Single enterprise USA placed License based Not for profit Business Model TO Publicly owned Globally and locally responsive Swiss placed ‘Fair share’ subscription based Not for profit Business Model The SNOMED SDO: What is this about?
The SNOMED SDO: Why a terminology? Terminologies Front office {citizens/patients} Read codes, SNOMED Individual conditions Exclusion categories “avoided” Records and communication Care and safety driven Codes Hierarchies Rapid change [days to weeks] Maps to classifications Classifications Back office {populations} ICD, OPCS (NIC) Group similar conditions Exclusion categories Statistical analysis Policy and strategy driven Codes Hierarchies Slow change [years] CLASSIFICATIONS AND TERMINOLOGIES HAVE DIFFERENT PURPOSES
Why a terminology? Precision K50 Crohns disease K51 Ulcerative colitis K52 Other non-infective gastroenteritis & colitis K52.0 Gastroenteritis and colitis due to radiation K52.1 Toxic gastroenteritis and colitis K52.2 Allergic & dietetic gastroenteritis and colitis K52.8 Other specified non-infective gastroenteritis and colitis K52.9 Non-infective gastroenteritis and colitis unspecified Excludes: Colitis, diarrhoea, enteritis, gastroenteritis Unspecified in countries where the condition can be assumed to be of infectious origin Functional diarrhoea Neonatal diarrhoea Psychogenic diarrhoea
Why a terminology? Accuracy K50 Crohns disease K51 Ulcerative colitis K52 Other non-infective gastroenteritis & colitis K52.0 Gastroenteritis and colitis due to radiation K52.1 Toxic gastroenteritis and colitis K52.2 Allergic & dietetic gastroenteritis and colitis K52.8 Other specified non-infective gastroenteritis and colitis K52.9 Non-infective gastroenteritis and colitis unspecified Excludes: Colitis, diarrhoea, enteritis, gastroenteritis Unspecified in countries where the condition can be assumed to be of infectious origin Functional diarrhoea Neonatal diarrhoea Psychogenic diarrhoea
Why a terminology? Myocardial infarction Heart attack Coronary thrombosis MI Myocardial infarct
Why a terminology? Safety Myocardial infarction Heart attack Coronary thrombosis MI Myocardial infarct Mitral incompetence Medial incisal Medical language = ambiguous
Why a terminology? Reduce ambiguity P Spinal cord compression SCord compression P Umbilical cord compression S Cord compression
Why a terminology? Reduce ambiguity P Spinal cord compression S Cord compression P Umbilical cord compression S Cord compression
Why a terminology?Record keeping • To aid their memory • To legally document what they saw & did (and sometimes why) • To communicate to other members of a team • To satisfy requirements of protocols & systems [secondary uses] • Research protocols • To support and justify reimbursement • Minimum data sets • Professional guidelines Why do clinicians record patient data?
Why a terminology?Record keeping • Secondary uses of clinical data are any uses other than the primary purpose [“direct patient care”] for which the data is recorded • ICD-9-CM coding for reimbursement can be derived from the dictated discharge summary, where the primary purpose may be documentation +/- communication, (not reimbursement). • Communicable disease reports to the health department can be derived from routine lab culture reports, where the primary purpose is communication to the ordering physician, (not epidemic detection). • Currently secondary uses largely involves human translation from patient record to secondary use data set
Why a terminology?Record keeping • THE IDEAL • Record clinical data once • with fidelity to the clinical situation • Allow systems to derive needed data from that single instance of recording Potential for financial savings and increased data accuracy
Why a terminology?Record keeping • THE REALITY • Clinicians find themselves entering the same basic clinical facts multiple times from slightly different perspectives for different purposes • Reimbursement coding skews clinical data • The level of detail is tuned to optimize reimbursement • Sometimes the clinical reality is obscured by lack of fidelity in the coding options available
Why a terminology?Record keeping • Terminology enables the ideal • Microbiology laboratories • positive Salmonella culture • Reports go to the physician(s) caring for the patient • Reports also go to local/state reportable disease registries Increasing data accuracy for policy and strategy as well as individual patient care
Why a terminology?Improving clinical care • Major driver for clinicians • Example; changing specific patients from one type of therapy to another • Search out all patients with Hypertension and/or cardiac failure who are on high sodium content antacids • Convert to low concentration antacid or alternative therapy Can only be done with EHR’s with a terminology and end user query tools
Why a terminology? Safety • Currently data transcribed repeatedly as it flows through the patient journey • The Joy Project • 10 out of 31 patients, 32% underlined a part of their record as incorrect. The origin of data error was investigated • 3 out of the 10 errors, 30% were attributed to: • i) manual data transcription error • 2 out of the 10 errors, 20% were attributed to: • ii) poor data entry • 1 out of the 10 errors, 10% could have been attributed to either i) manual data transcription or ii) poor data entry. • 4 out of the 10 errors, 40% were attributed to other factors.
Why a terminology? Clinical Innovation • Safety and Efficacy Register of New Interventional Procedures {SERNIP} • New interventions registered with professional body who ask for SNOMED concept • Enables the efficacy, effectiveness, of new procedures to be monitored and educational components addressed by professional bodies
Why a terminology?Link to knowledge services • Knowledge bases can be tagged with a standard terminology through: • Automatic tagging software and/or • Manual highlighting of concepts • Through appropriate software the clinician can then access appropriate knowledge for the precise clinical problem • It also is a potentially valuable tool for patients
Why a terminology?Link to ‘grey literature’ services • SNOMED enables Reuters to categorise medical stories and provide information specific to Client’s interests • Tagging a story takes ‘less than two minutes’ • Improved citizen access and clinician awareness to world health news
Why a terminology?Rapid clinical responses • Health records encoded with a standard terminology mean that when drug safety alerts are issued the GP can search out all their patients on drug x and take appropriate action • No unnecessary delays or resource wastage on hand searching through records or awaiting patient reactions
Why a terminology?Decision support • Reminder and recall service for cervical screening and immunisation • Drug-drug interaction • Drug- clinical condition interaction • Investigation- clinical condition interaction eg pacemaker in situ and Magnetic Resonance Image scans
Why a terminology?Clinical Audit • Part of professional practice to maintain registration in UK • Is the reality of practice meeting current levels of knowledge • Example: Have all the patients taking the drug Amiodarone had their Thyroid function measured? Use of terminologies in EHR’s greatly enables clinical audit
Why a terminology?Payment on clinical outcomes • General Practitioners in England currently paid on the quality of their care through 21 rule sets • Basis is Read Codes plus published evidence eg National Institute of Excellence {NICE} • Example: Indicator ASTHMA 8: The percentage of patients aged eight and over diagnosed as having asthma from 1st April 2006 with measures of variability or reversibility.
Why a terminology?Sharing the record with the patient Headline: 'Hospital that forgot to tell nurse she had cancer' Sub-headline '£100, 000 for woman who thought she had escaped illness' 'Doctors failed to tell a nurse they suspected she had breast cancer for two years. Jayne Muir 50 discovered their suspicions only from reading about it in her medical notes. A mammogram had shown she could have cancer.......by the time she was diagnosed the cancer had spread dramatically' Page 23; 29th October 2005: Daily Mail Julie Weldon Science Correspondent Sharing records is easier with EHR’s encoded with a terminology; Two new UK projects
Why SNOMED CT? • Directly supports • Representation & queries based on meaning • Computable tracking of historical relationships of retired codes • Indirectly supports • Specification of user interface • Definition of minimum data sets, checklists, and data collection standards
Why SNOMED CT? • Provides a common representation • Independent of how the data was recorded: • natural language • e.g. English, French, Spanish, ... • terms • e.g. craniopharyngioma, Erdheim tumor, pituitary adamantinoma, Rathke's pouch tumor • data sets • information system interface • implementation details • type of site • type of user
Why SNOMED CT? • First rule of coding: Yesterday’s data should be usable tomorrow • Non-Hodgkin’s lymphoma histologic type • Classification has been changing • More than 25 different classifications have been published since 1925 • Major classifications in past 30 yrs: • Rappaport • Working Formulation • Kiel • REAL • WHO SNOMED CT Manages Obsolescence
Acute lymphoblastic leukemia ICD-O-3 ICD-O-2 Acute lymphoblastic leukemia L1 L2 L3 • Acute lymphoblastic leukemia • Precursor B cell leukemia • Burkitt cell leukemia M-98363 M-98213 M-98263 M-98283 M-98263 SNOMED history table contains two rows: M-98213 REPLACED-BY M-98363 M-98283 REPLACED-BY M-98363
Why SNOMED CT?Subsets • A collection of terminology, selected and grouped for a particular purpose • May be composed of anything from a single component to the entire set of concepts, descriptions or relationships • Commonly needed for: • Data quality improvement • Message field validation • Simplified data entry and retrieval • Elimination of ‘noise’
Why SNOMED CT? Subsets • Subsets are an integral part of SNOMED CT • SNOMED CT is a large, rich and complex resource • The subset mechanism provides a consistent way to make this rich content manageable • Subsets assist implementation of appropriate, usable, and consistent interfaces through which users can access relevant concepts • Subsets allow clear and concise expression of value-set constraints for data entry and communication specifications • The SNOMED CT subset mechanism provides a published common form for representation of subsets • This allows • A vendor neutral distribution format for subsets • Opportunities for alternative collaborative tooling to create and manipulate subset to meet global, national and local needs
Why SNOMED CT? Subsets • Devolved responsibility • National control • Provide effective tools: • Simple to use and individually configurable to allow subsets to be created/edited with the minimum of effort (including tutorials) • Ability to set permissions/rights to allow viewing and/or editing rights • Workflow elements • The tool must support multiple synchronous users • To support the distributed working environment it must be possible to undertake all of the above processes over the www
Why SNOMED CT? Team Based Care {UK view} 4 Byte set primary care clinical summary Version 2 acute sector clinical summary CTV3 all sectors specialist & generalist full clinical record SNOMED CT all sectors specialist & generalist full clinical record multi-national
Why SNOMED CT? • Most comprehensive terminology • Humphreys BL et al JAMIA 1997;4:484-500 • Scores higher than alternatives on independent multidimensional evaluation • Ref provided in pack • Dynamic twice yearly releases • Multiple hierarchies for consistent retrieval and analysis • Cross referenced to multiple classifications
What will SNOMED NOT do? • How far does a SNOMED CT take us towards being able to use secondary data? • Permits common reference points for meaning • With appropriate history mechanism, sustains the value of previously recorded data • Does not (independently) solve the problem of data collection / data entry
What will SNOMED NOT do? • It will not on its own solve the professional data input challenges of accuracy • Who is responsible for defining professional standards of data quality? • Will professional specialty organizations step up to the challenge? • What clinical data is essential? • Who decides so that clinicians are not overburdened? • How can support and incentives be provided to clinicians? SNOMED CT can act as a support tool to these bodies
What will SNOMED NOT do? • It will not solve your legacy data and legacy system problems BUT will offer some help through mappings
What will SNOMED NOT do? • It will not on its own solve the secondary use dilemma • The value of secondary data accrues (mainly) to parties other than those who collect it • The value of secondary data depends on its quality, while the quality of data is directly proportional to the care with which it is collected SNOMED CT does enable the dilemma to be mitigated
SNOMED CT (in the NHS) will facilitate the sharing of electronic patient records to provide clinical support across all care settings SNOMED CT is part of the solution, not part of the problem….. In conclusion….
The SNOMED StandardsDevelopment Organization • The Value Proposition • Context and Benefits • Governance and Structure • SSDO Financial Model • Technology Environment • Code of Conduct and Benefit Summary • Process for Moving Forward
What is theSNOMED Terminology? • Documents describing the SNOMED CT standards and specifications • The terminology database consisting of • Concepts, Descriptions, Relationships • Technical tools to support development and request processing