Download
1 / 78
780 likes | 934 Views
SARS “Outbreak” on a University Campus. Management of a Confirmed Severe Acute Respiratory Syndrome Case at the University of North Carolina at Chapel Hill. Peter A. Reinhardt, Director Mary C. Crabtree, Workplace Safety Manager Department of Environment, Health & Safety. About SARS.

E N D
SARS “Outbreak”on a University Campus Management of a Confirmed Severe Acute Respiratory Syndrome Case at the University of North Carolina at Chapel Hill Peter A. Reinhardt, Director Mary C. Crabtree, Workplace Safety Manager Department of Environment, Health & Safety
About SARS • Case definition • Fever of 100.4 F or greater (how it usually begins) • Respiratory symptoms (e.g., dry cough, shortness of breath; may develop after 2-5 days) • Travel to affected area or exposure to someone with SARS • Viable up to 72 hours in the environment • Develops into pneumonia, observable on a chest X-ray. 10% mortality from respiratory failure. • International epidemic. Cases from 1 November 2002 to 31 July 2003: • 8,098 cases worldwide • 774 deaths • In U.S., 74 Probable cases as of 31 July 2003, with no deaths or secondary transmissions within the U.S. Testing has been limited—only 8 cases have been confirmed by the CDC.
Where Did SARS come from? • A number of initial cases were food handlers, so the epidemic may have started with them. • Researchers were able to detect the SARS virus in two species found in local food markets. • The virus may have been initially transmitted to man from those species (zoonosis). • Those species may have acquired the virus from more exotic species
About SARS • Routes of transmission: Direct contact (within three feet)—especially from cohabitation or in healthcare facilities. Work colleagues or others in the waiting room are not considered close contacts. • Incubation period: Usually 5-7 days, but up to ten days. Some reports of 13-16 days. • Control measures: Avoid endemic areas and their healthcare facilities. Avoid direct contact with a person who has SARS. • 100% protection of healthcare workers if proper PPE is used: properly fitted N-95 respirators, gloves, goggles and gown.
Treatment for SARS • Currently, there is no treatment for SARS. • Therefore, the symptoms (e.g., cough, fever) are treated and, hopefully, lessened. • Due to the high risk of transmission in a healthcare setting, confinement in a healthcare facility is not indicated. Instead, patients are isolated at home unless respiratory symptoms necessitate hospitalization. 50% of the SARS cases in Singapore and Toronto were healthcare workers. • Symptoms of residential patients are monitored frequently, and their environment is disinfected frequently. • Family members/cohabitants are isolated with the patient, and their symptoms are also frequently monitored.
Tests for SARSexpensive, new, limited capacity • Can’t afford to test everyone with a fever or respiratory symptoms. • Rule out tests—influenza and mycoplasma. • “Atypical pneumonia,” which is not uncommon, and for which there are no rule out tests, is very difficult to distinguish from SARS. • Detection of antibodies in serum—usually develop 8-10 days from illness onset, but sometimes not until 28 days. • PCR—like serology, is sensitive and specific, but not definitive early in the illness. • Lung sample from autopsy • Detection of antibodies in lung tissue (most accurate) • Histopathology via electron microscopy (characteristic tissue damage or virus morphology) • Confirmatory tests (multiple tests, methods, labs) is critical before identifying an index case.
UNC’s Contingency Planning for SARSSpring 2003 • Establish a UNC SARS website, with recommendations, policies and informational links. • Key administrators meet to decide University travel policies and communications for students, faculty, staff and visitors. • Meeting of the University Emergency Warning Committee. • Emails and Gazette (employee newsletter) article to inform travelers prior to the end of the semester.
UNC-Chapel Hill Travel Guidance • Monitor WHO, CDC and State Department advisories and, when they differ, err on the side of caution by following the most conservative advice. • No UNC employee or student is required to travel to an area where a travel advisory or alert is in effect. • Travelers from an affected area must monitor their health for SARS symptoms for at least 10 days after departure. Take your temperature daily. • At the first sign of a fever or respiratory problems, telephone a healthcare provider for advice and to arrange a medical evaluation. • Special announcement at May 2003 commencement.
Laws of Risk Communication High Perceived Risk • Exotic/new • Not knowable/uncertain • Controlled by others • Coerced • Catastrophic • Immediate effect • Dreaded Other variables include responsiveness, openness and trust. In general, more information (rather than less) and taking action improves relations.
Response to UNC Travel Guidance “Married student housing is a hotbed of international travel to known SARS areas. One neighbor is planning a trip to Toronto and another is currently traveling in Taiwan, Vietnam, and other known SARS areas. Is anything being done as far as surveillance? There seems to be very little regard among the Asian community regarding the problem of SARS and travel to areas where the epidemic persists. Please advise.” “What are you doing to protect my daughter from SARS? Telling people who have traveled in ‘affected’ areas to ‘take their temps’ isn't good enough for me. I think you should be monitoring these students for the incubation period when they come back to campus to keep all the students safe.”
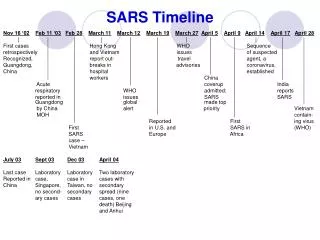
Timeline of SARS on Campus 3 June 2003: North Carolina reported its ninth case of suspected SARS, an Orange County man, to the Centers for Disease Control and Prevention (CDC). Thursday 5 June 2003: 9:30 a.m. UNC first informed that suspect SARS case had worked as a contactor at UNC 21-23 May while asymptomatic. Case became symptomatic on 24 May, so risk to UNC staff was deemed to be very small or none. • Orange County Public Health (OCPH) interviews three coworkers with closest contact, as reported by the index case. • OCPH drafts letter to coworkers, describing current knowledge and activities. • OCPH letter distributed via email to 325 staff in building in which index case worked. • UNC Emergency Warning Committee meets. An informational email is drafted to all faculty and staff for distribution that night.
Information Provided by OCPH to Employees • “Potential SARS suspect.” • “Symptoms developed after [5/23, his last day at UNC]. The potential for transmission without symptoms is very low.” • “It is now beyond the ten day incubation period.” • But…“Should you develop any of these symptoms, contact a healthcare provider and advise them of your possible exposure to a SARS patient.”
Potentially Affected UNC Staff • Three individuals with closest, longest contact • About 250 employees in the Giles Horney Building • About 200 Facilities Services and Planning and Construction Staff (150 of whom receive email) • 40 Administrative Technical Network staff • 135 Energy Services employees in Electrical Distribution, COGEN and North Chiller Plant
Employee Response to Initial Notice “Where’s Giles Horney? Was he on campus? Was he in my building?” “Has he been seen at UNC Hospitals? Is it safe to go there?” “A number of people have been sick here in the Giles Horney Bldg (who came in contact with this individual) before, during and after Memorial Day. I was sick the entire holiday weekend and beyond and so was one of my coworkers. “Numerous people were sick the following week, etc. This individual even ate with all of us during an employee luncheon. “I really think the University should close this building down and disinfect it. Also, why wasn't that done last weekend since we finally received information on 6/5/03.”
Friday 6 June 2003 • Suspect case was reclassified as “probable.” • EHS, Student Health Service and UNC Hospitals plan daily teleconferences, starting on Tuesday 10 June at 8 a.m.
Public Health Interests and Activities • Vigilantly prevent SARS outbreak—monitor for any sign of a secondary transmission. • Practice epidemiology according to specific rules and procedures: • Identify cases and interview high-risk contacts. Be prepared to order quarantine and isolation, when necessary. • Preserve case privacy • Inform local healthcare facilities of risk and precautions • Providing public information about risks and precautions. Established public information line 14 June. • Prevent panic; reassure public. • Recognize that employer responsibilities may differ. • Concerned about implications to other affected parties and setting precedent.
University Interests • Health and safety of its students, faculty, staff and visitors • Contingency planning for best and worst case scenarios • Employee relations • Student and parent relations • Business continuation for UNC Hospitals and the University
UNC Hospitals Interests • Avoid experiences of hospitals in Asia and Toronto: • Prevent SARS transmission to hospital staff, visitors and other patients—protect hospital facilities and staff. • Prevent disruption of hospital clinics and services due to hospital outbreak control measures—preserve capacity to continue business of treating patients. • Prevent from being labeled as a “SARS Hospital” with commensurate damage to reputation and business. • Because so much is at stake, contingency planning for the reasonable worst case—a community outbreak. If an outbreak were to occur, UNC Hospitals must be ready to respond, rather than being incapacitated in managing SARS among its healthcare workers.
UNC Hospitals Protective Measures-Monday 9 June • Signs on all doors, advising SARS-risk patients to go to the emergency department’s external door. • Post guard at emergency department’s external door with surgical masks for potential patients. • Development of internal policy and procedures for SARS-suspect patients, including staff PPE requirements. • Directive to medical staff to get fit-tested • UNC Hospitals employees are fit-tested by Hospital • Physicians are UNC faculty, and are fit tested by University Employee Occupational Health and campus Environment, Health and Safety
UNC Hospitals Protective Measures-Monday 9 June • Establish special examination entrance and rooms. • Preparation of isolation rooms in the Hospital. • In case of epidemic, begin search for off-site screening facility. Considered locations included: • Student Health Center (near UNC Hospitals) • Football stadium first aid station • Parking areas near Giles Horney
Monday 9 June 2003 • EHS clears schedule at University Employee Occupational Health Clinic (UEOHC) to fit test identified healthcare providers anytime during that week. • Afternoon: After CDC laboratory tests were positive, the case was reclassified to “confirmed.”
Handling SARS Calls from the University and Community • In the evening of Monday 9 June, an update email was sent to all UNC employees with the news that the case was “confirmed” and directed all information phone lines into UNC Hospitals HealthLink. • The important message is: “Unless there is an emergency, call HealthLink. If you are symptomatic, do not go to a healthcare facility without calling first.” • Community practices in Chapel Hill follow suit and referred SARS queries to HealthLink • UEOHC, Student Health Service and OCPH also handled many calls. • Calls received by Chamber of Commerce: “Is it safe to travel to Chapel Hill?”
UNCH HealthLink • Added staff to handle SARS calls, including questions during daytime working hours—when normally they just make appointments. • Referred worried well to information sources, the University Employee Occupational Health Clinic (UEOHC) or their primary provider. • Referred symptomatic, potentially exposed callers to Infectious Disease for a phone evaluation. If necessary, arrange for examination at special examination entrance and rooms. • When established, would refer symptomatic, potentially exposed callers to off-site screening facility.
Questions of Concerned Peoplecalls and emails to EHS “My staff and I pick up car fleet keys at the building. Should we use masks when entering the building? Are there chances of being infected via the use of a fleet vehicle?” “Staff from the building are frequently in my building. Do they pose a risk to me?” “I am concerned that a coworker frequently visits the building, yet has not been included in the potentially exposed group. I am also concerned because my job puts me all over campus and I could unknowingly become a vector to the rest of campus.” “My daughter is scheduled for freshman orientation on campus next week. Will she be safe?”
Tuesday 10 June 2003 • Investigation begins on two “special interest” cases: an Orange County man seen as an outpatient at Duke University Medical Center (Durham County), and a Wake County man at Western Wake Medical Center. Both are UNC employees who worked in the same building as the SARS index case. • At UNCH request, State Division of Public Health initiates a daily teleconference for public health, UNCH, and University technical staff.
Tuesday 10 June 2003 • UNCH stations security guards to entrances of its hospitals and clinics • Meeting of 150 Giles Horney employees. • County and State Public Health Officials invited to attend and answer questions. • Upon hearing reports of recent employee illnesses, State Division of Public Health commits to a health questionnaire for potentially exposed employees.
Good Questions about SARSat the Tuesday 10 June employee meeting “I’ve heard SARS is a virus similar to the common cold. The CDC lists personal contact as the suspected transmission method, but there is no mention of transmission from cough droplets on furniture, etc. Is SARS transmitted environmentally, like the common cold?” “Can an asymptomatic patient transmit the disease?” “Can a person get a mild case of SARS? If so, are they infectious to others?” Among the technical experts and medical professionals, uncertainty about these issues created dissonance and raised their perception of the public health risks.
Toronto Interests • Local economy • Reputation and public relations • Is Toronto exporting SARS? • Are Toronto healthcare facilities taking appropriate precautions to stop the spread of SARS? • Local Canadian Health Official on 11 June: “Case defies the accepted understanding of the disease and method of spreading” • Avoidance of a WHO or CDC travel alert or advisory
Wednesday 11 June 2003 • Consideration of temporarily closing Giles Horney was tabled by the UNC Emergency Warning Committee due to concern that: • If some employees had SARS, they would be dispersed to towns and counties less prepared to identify and contain SARS. • How would UNC and UNCH continue its operations without Giles Horney and its facilities services? • Pre-work temperature monitoring procedure discussed and adopted. EHS orders 400 digital thermometers overnight. • UNC Hospitals, EHS and UEOHC proceeds with plans for temporary screening facility, with Giles Horney employees becoming their primary concern. • EHS orders N-95 respirators. (UNCH had one month supply for 24hr call.)
Thursday 12 June 2003 • 8 a.m.: At UNCH Grand Rounds, physicians ask, “Why isn’t UNC closing Giles Horney?” • 3 p.m.: UNC and UNCH decides on the site of screening facility: • Park and Ride lot near Giles Horney not used during that time of year. • Public availability, if necessary. • Employee screening is not sanctioned by OCPH as a public health action. • EHS prepares mobile fit-testing facility and continues search for N-95 respirators.
Employee Meeting Thursday 12 June • Presentation by Chancellor Moeser • Announce, begin temperature program • David Weber, M.D., announced screening facility • SPH Dean Roper and PH Director discussed risks, answered questions • Discuss cleaning the building • Distribute health questionnaire
Should We Clean the Giles Horney Building? • Many employees demanded that we clean the building. Several administrators supported this. • Public health officials told us that there is no environmental SARS risk. Cleaning the building was unnecessary, of no material benefit, and would set a bad precedent for other affected parties (i.e., the confirmed case’ primary doctor’s office). It would cause undue community concern and provide false assurances to employees. • Although SARS virus viability is only 72 hours, could virus be present if people in the building had “mild” case of SARS? • Practical problems: No standards for cleaning buildings. How clean is clean? Where are the boundaries for cleaning? • Consideration of a “peace of mind” cleaning.
Friday 13 June 2003 • Screening facility opens at 7 a.m. in tents erected overnight. • UNC Hospitals prepares for lockdown of all hospital and clinic entrances. • EHS continues distribution of surveys and thermometers.
Screening Facility • To screen employees and family with symptoms. Capacity of about 6-12 persons per hour. Conveyance to UNC Hospitals, if necessary. • Multiple stations: • Registration • History and counseling • Physician evaluation • Portable chest X-ray • About 40 staff: • UNCH: screening (5), nurses (4), radiation technician (1), medical technician (1), UNCH EHS (2), Van shuttle (1), Ground transport to Carolina Air Service (2) • UNC Physicians (4-5) • UNC Facilities Services (5) • UNC School of Nursing volunteers (5) • UNC EHS: reception (1), fit testing (3) radiation safety (2) • UNC Public Safety (2) • UNC Employee relations staff present to meet with employees • It was handled extremely well and did not become the media circus that CDC feared.
Screening Facility Site Preparation by UNC Facilities Services Thursday 12 June, 3 p.m.: Informed of need to a) set up black-out fencing and tents in park-and-ride lot near Giles Horney, b) procure fencing materials. 4 p.m.: Begin fence construction. 7 p.m.: Completed the installation of black-out fence. (Kept media at bay.) Friday 13 June, 5 a.m.: Housekeeping delivery and set up of tables and chairs. 6 a.m.: Install wiring and receptacles. Install air conditioning for inflatable tents, powered by generators rented from Wilmington. 8 a.m.: Install locally purchased pop-up tents, water coolers, interior lighting and trash receptacles as needed. 9 a.m.: a) Sent mechanic to Garner to pick up domestic water storage tank, b) procured pump to supply domestic water, c) assembled and set temporary towel and hand sanitizer dispensers. 2 p.m.: Water pump and tank was set up and tied into hand washing sink.
Screening Facility Site Preparation by UNC Hospitals • Tents, ordered overnight, erected with help of UNC Facilities Services: • 3 inflatable tents from Charlotte Fire Dept., delivered 9 p.m. on 12 June. • “Decon” tents from OCPH • Waiting area tents from UNC • Thermometers, sphygmomanometers, etc. bought overnight from Wal-Mart and area pharmacies. Gloves, gowns, etc. from UNCH Central Distribution. • Rental trucks to hold supplies. • T1 connection by mid-day.
Screening Facility Site Preparation by University EHS • For registration, created a report from EHS’ information system (HASMIS) of employee basic demographics and medical record numbers. • Provided greeter/reception staff. • Established and staff a mobile fit-testing facility. • Procured of additional N-95 respirators. • Established external shielding for portable X-ray unit.