Download
1 / 1
10 likes | 91 Views
Complete Cytoreduction of Advanced Ovarian Malignancy using Neutral Argon Plasma. Madhuri TK , Tailor A , Butler-Manuel SA Department of Gynaecological Oncology Royal Surrey County Hospital, Guildford, UK. Introduction

E N D
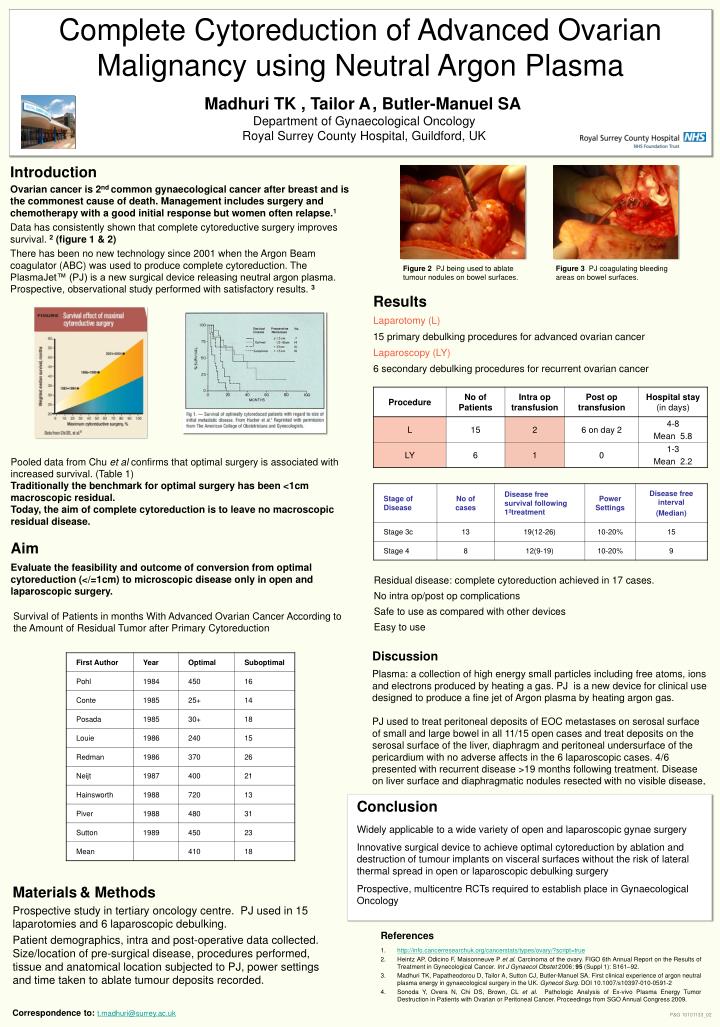
Complete Cytoreduction of Advanced Ovarian Malignancy using Neutral Argon Plasma Madhuri TK, Tailor A, Butler-Manuel SADepartment of Gynaecological OncologyRoyal Surrey County Hospital, Guildford, UK Introduction Ovarian cancer is 2nd common gynaecological cancer after breast and is the commonest cause of death.Management includes surgery and chemotherapy with a good initial response but women often relapse.1 Data has consistently shown that complete cytoreductive surgery improves survival. 2 (figure 1 & 2) There has been no new technology since 2001 when the Argon Beam coagulator (ABC) was used to produce complete cytoreduction. The PlasmaJet™ (PJ) is a new surgical device releasing neutral argon plasma. Prospective, observational study performed with satisfactory results. 3 Figure 2 PJ being used to ablate tumour nodules on bowel surfaces. Figure 3 PJ coagulating bleeding areas on bowel surfaces. Results Laparotomy (L) 15 primary debulking procedures for advanced ovarian cancer Laparoscopy (LY) 6 secondary debulking procedures for recurrent ovarian cancer Pooled data from Chu et al confirms that optimal surgery is associated with increased survival. (Table 1) Traditionally the benchmark for optimal surgery has been <1cm macroscopic residual. Today, the aim of complete cytoreduction is to leave no macroscopic residual disease. Aim Evaluate the feasibility and outcome of conversion from optimal cytoreduction (</=1cm) to microscopic disease only in open and laparoscopic surgery. Residual disease: complete cytoreduction achieved in 17 cases. No intra op/post op complications Safe to use as compared with other devices Easy to use Survival of Patients in months With Advanced Ovarian Cancer According to the Amount of Residual Tumor after Primary Cytoreduction Discussion Plasma: a collection of high energy small particles including free atoms, ions and electrons produced by heating a gas. PJ is a new device for clinical use designed to produce a fine jet of Argon plasma by heating argon gas. PJ used to treat peritoneal deposits of EOC metastases on serosal surface of small and large bowel in all 11/15 open cases and treat deposits on the serosal surface of the liver, diaphragm and peritoneal undersurface of the pericardium with no adverse affects in the 6 laparoscopic cases. 4/6 presented with recurrent disease >19 months following treatment. Disease on liver surface and diaphragmatic nodules resected with no visible disease. Conclusion Widely applicable to a wide variety of open and laparoscopic gynae surgery Innovative surgical device to achieve optimal cytoreduction by ablation and destruction of tumour implants on visceral surfaces without the risk of lateral thermal spread in open or laparoscopic debulking surgery Prospective, multicentre RCTs required to establish place in Gynaecological Oncology Materials& Methods Prospective study in tertiary oncology centre. PJ used in 15 laparotomies and 6 laparoscopic debulking. Patient demographics, intra and post-operative data collected. Size/location of pre-surgical disease, procedures performed, tissue and anatomical location subjected to PJ, power settings and time taken to ablate tumour deposits recorded. • References • http://info.cancerresearchuk.org/cancerstats/types/ovary/?script=true • Heintz AP, Odicino F, Maisonneuve P et al. Carcinoma of the ovary. FIGO 6th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet 2006; 95 (Suppl 1): S161–92. • Madhuri TK, Papatheodorou D, Tailor A, Sutton CJ, Butler-Manuel SA. First clinical experience of argon neutral plasma energy in gynaecological surgery in the UK. Gynecol Surg. DOI 10.1007/s10397-010-0591-2 • Sonoda Y, Overa N, Chi DS, Brown, CL et al.Pathologic Analysis of Ex-vivo Plasma Energy Tumor Destruction in Patients with Ovarian or Peritoneal Cancer. Proceedings from SGO Annual Congress 2009. Correspondence to: t.madhuri@surrey.ac.uk P&G 10101133_02