Download
1 / 62
700 likes | 997 Views
Antithyroid Drugs. Dr Muhammad Omar Jamil , M.D. Management of Hyperthyroidism. Medical therapy with antithyroid drugs such as propylthiouracil or methimazole Ablation of the thyroid gland with radioactive iodine Subtotal<br>ear total thyroidectomy thyroidectomy.

E N D
Antithyroid Drugs Dr Muhammad Omar Jamil, M.D
Management of Hyperthyroidism • Medical therapy with antithyroid drugs such as propylthiouracil or methimazole • Ablation of the thyroid gland with radioactive iodine • Subtotal\near total thyroidectomy thyroidectomy
Self-limited causes of hyperthyroidism, such as subacutethyroiditis, iodine-induced hyperthyroidism, and exogenous administration of T4, can be treated symptomatically. For more significant cardiovascular symptoms, beta-adrenergic blockade with propranolol can be helpful.
Anti-thyroid Drugs • thioamides • iodides • radioactive iodine • beta adrenoceptor blocking agents
Thioamides • Methimazole 5mg; Propylthiouracil (PTU) 50mg; Carbimazole 5mg, 20mg • MOA: • contain a sulfhydryl group and a thiourea moiety withina heterocyclic structure • inhibit synthesis by acting against iodide organification (both) • coupling of iodotyrosines (both) • blocks conversion of T4 to T3 (PTU)
Thioamides • immunosuppressive effects: 1) Decrease the antithyrotropin-receptor antibodies 3) soluble interleukin-2 and interleukin-6receptors decrease with time
Thioamides • may induce apoptosis of intrathyroidal lymphocytes, and decrease HLA class II expression • circulating suppressor T cells • helper T cells, natural killer cells and activated intrathyroidal T cells • analysesof animal data and human studies suggestedthat changes in the immune system may not be predicated solelyon changes in thyroid function.
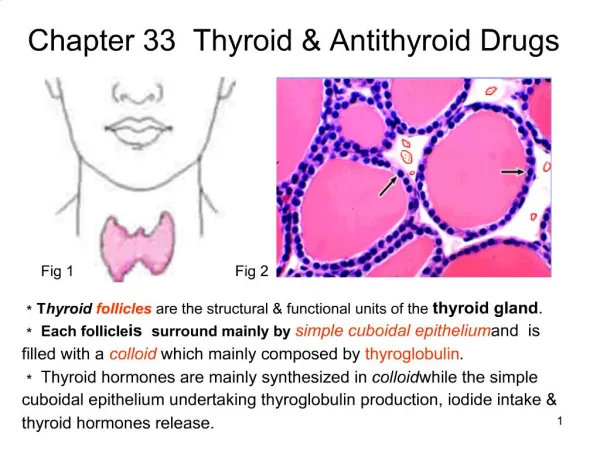
Effects of Antithyroid Drugs. inhibition of thyroid hormone synthesis and a reduction in both intrathyroidal immune dysregulation and the peripheral conversion of T4 to T3. Tyrosine-Tg denotes tyrosine residues in thyroglobulin, I+ the iodinating intermediate, TPO thyroid peroxidase.
Synthesis of Thyroxine and Triiodothyronine. In Panel A, thyroid peroxidase (TPO), a heme-containing glycoprotein, is anchored within the thyroid follicular-cell membrane at the luminal side of the thyroid follicle. In Panel B, the first step in thyroid hormone synthesis involves generation of an oxidized enzyme promoted by endogenously produced hydrogen peroxide. In Panel C, the oxidized enzyme reacts with trapped iodide to form an "iodinating intermediate" (TPO–Iox), the nature of which is not entirely understood. Some investigators favor the formation of a heme-linked iodinium ion (TPO–I+), whereas others suggest the formation of hypoiodite (TPO–O–I–).
.Panel D, in the absence of an antithyroid drug, the iodinating intermediate reacts with specific tyrosine residues in thyroglobulin (Tg) to form monoiodotyrosine and diiodotyrosine. Subsequent intramolecular coupling of MIT and DIT forms triiodothyronine, and the coupling of two DIT molecules forms thyroxine. In the presence of an antithyroid drug (e.g., methimazole, shown in Panel E), the drug serves as an alternative substrate for the iodinating intermediate, competing with thyroglobulin-linked tyrosine residues and diverting oxidized iodide away from hormone synthesis. The drug intermediate with a sulfur-linked iodide is a theoretical reaction product.6 In Panel F, the oxidized drug forms an unstable drug disulfide7 that spontaneously degrades to an inactive desulfurated molecule, shown as methylimidazole. Antithyroid drugs also impair the coupling reaction in vitro, but it is uncertain whether this occurs in vivo.
Thioamides • Methimazole and carmimazole: 10-20mg 8-12hours (titration: 2.5-10mg) • PTU: 100-200mg 6-8hours (titration: 50-100mg) • requires a long period of treatment (12-18 months) • 50-68% incidence of relapse • Labs assessed every month
Thioamides • Pharmacokinetics: • almost completely absorbed in the GIT • rapidly absorbed fromGI tract • peak within one to twohours • Serum levels have little todo with antithyroid effects, which typically last from 12 to24 hours for PTU • methimazole long duration once-daily
Clinical Pharmacology • serum half life: 90mins(PTU) ; 6 hours (methimazole) • excretion: kidney – 24 hours (PTU) ; 48 hours (Methimazole) • can cross placental barrier (lesser with PTU) • Methimazole 10x more potent than PTU • PTU more protein-bound
Clinical Pharmacology • doses do not need tobe altered in children ,elderly, renalfailure and liver disease, although the clearance of methimazole (butnot PTU) may be decreased.
Clinical Use of Drugs • two ways: primarytreatment for hyperthyroidism or preparative therapy beforeradiotherapy or surgery • Graves'disease, "remission“ is possible. (euthyroid for one year after cessation) • notprimary therapy for toxic multinodular goiters and solitary autonomous nodules,because spontaneous remissions rarely occur
Clinical Use of Drugs • primary treatment in pregnant and most children and adolescents • preferable in severe Graves' eye disease • radioiodine therapy has been associated with worsening ophthalmopathy
severe Mild to moderate eye Radioiodine may be preferable as initial therapy for adults in the United Statesbut not for those in the rest of the world. I
Clinical Use of Drugs • antithyroid drugs,radioiodine, and surgery :patient satisfaction > 90% • costs lowest : drug • also used to normalize thyroid function before the administrationof radioiodine, caused by a rise in stimulating antithyrotropin-receptorantibodies
Choice of Drugs • methimazole>PTU, by better adherence and more rapid improvement in T3 and T4, and side-effect • propylthiouracil : during pregnancy.
Practical Considerations • starting dose of methimazole : 15 to 30 mg qd, • PTU : 300 mg daily tid • many patients can be controlled with smaller doses of methimazole,suggesting that the accepted potency ratio of 10:1 for methimazoleas compared with PTU is underestimated . • if methimazole is overly aggressive iatrogenic hypothyroidismwith relatively mild hyperthyroidism may result
Practical Considerations • follow-upevery four to six weeks,until thyroid function is stable or the patient becomeseuthyroid • Maintenance : 5 to 10 mg of methimazole or 100 to 200 mg of PTU daily. • hypothyroidism or goiter can develop if the doseis not decreased appropriately
Practical Considerations • After the first three to sixmonths, follow-up intervals can be increased to every two tothree months and then every four to six months. • Serum TSH levels remain suppressed for weeks or even months, despite anormalization of thyroid hormone levels, so a test of TSH is a poor early measure
Practical Considerations • patients sometimescontinue to have elevated serum T3 levels despitenormal or even low T4 or FT4, increase, not decrease, the antithyroid drug dose
Low Remission • severe hyperthyroidism • large goiters • T3-to-T4 ratio >20 • higher baselinelevels of antithyrotropin-receptor antibodies
Remission • age, sex, and smoking • Ophthalmopathy • duration of symptoms beforediagnosis • risk factors for relapse depression,hypochondriasis, paranoia, mental fatigue after an average ofthree years of antithyroid-drug therapy
Remission • TSHR at the end of a course oftreatment predictive value -->positive : relapse often • However, even thosepatients whose antibody titers have normalized have a fairlyhigh rate of relapse (30 to 50 percent)
Remission • Since immunosuppressive effects, a higherdose or longer treatment duration might enhance the chancesof remission. • prospectivetrials >4y follow-up do not indicate thattreatment for >1 year has any effect on relapserates • treatment for 12to 18 months is the usual practice
Discontinuation of Drug Treatment • relapse is increased in normalFT4 and T3but suppressedTSH. • Relapse usually occurs within thefirst three to six months after medication is stopped
Discontinuation of Drug Treatment • overall recurrence rate 50 to60 percent. • About 75 percent of women in remission whobecome pregnant will have a postpartum relapse of Graves' diseaseor the development of postpartum thyroiditis.
Discontinuation of Drug Treatment • When used before radioiodinetherapy, PTU (but not methimazole), increases thefailure rate of the radioactive iodine • This "radioprotective"effect of PTU may be related to its ability toneutralize iodinated free radicals produced by radiation exposure,can be overcome by increasing the radioiodine dose.
Side Effects • methimazole are dose-related, (PTU less clear ) • cutaneous reactions (usually urticariaor macular rashes), arthralgia, and GI upset 5% of patients, with equal frequencyfor both drugs
Side Effects • cross-reactivity between the twoagents may be as high as 50 percent. the use of thealternative antithyroid drug is contraindicated • arthralgias, should prompt drug discontinuation, : may be a harbinger of a severe transient migratorypolyarthritis known as "the antithyroid arthritis syndrome”
Side Effects Agranulocytosis • an absolutegranulocyte count of less than 500 per cubic millimeter • 0.37 % in PTU and 0.35 % methimazole • must bedistinguished from the transient, mild granulocytopenia (<1500 per cubic millimeter) in Graves' disease, African descent, and occasionally in patients treated with antithyroiddrugs. • baseline differential white-cell count
Side Effects Agranulocytosis • Occur within 90 daysof treatment, but can occur >1 year • greater in olderpatients • A higher rate of death • can develop after a prioruneventful course, a relapse and a second course of therapy.
Side Effects • Fever and sore throat are the most common • sepsis :very rapid onset of fever, chills, and prostration • Pseudomonas aeruginosa most common • G-CSF may shorten the time to recoveryand length of hospitalization
Side Effects • Hepatotoxicity 0.1 to 0.2 % • 30 % with normalbaseline GPT treated with PTU,transient increases ranging from1.1 to 6 times normal —resolve while therapy is continued. • asymptomatic elevationsin GPT occur frequently in untreatedpatients with hyperthyroidism and are not predictive of furtherincreases after PTU therapy.
Side Effects • The average duration of PTU therapy before theonset of hepatotoxicity is approximately three months • allergic hepatitis • Pathology: submassive ormassive hepatic necrosis • case fatality rate of 25 to 50 % • Liver transplantation may be required
Side Effects • methimazole andcarbimazole are typical of a cholestatic process • alternative agentcould be used cautiously
Side EffectsVasculitis • PTU >methimazole • drug-induced lupus • perinuclearantineutrophilcytoplasmic antibodies, antimyeloperoxidaseantineutrophilcytoplasmic antibodies. • Mechanism: PTU can react with myeloperoxidase to form reactiveintermediates promote autoimmune inflammation
Side EffectsVasculitis • acute renal dysfunction,arthritis, skin ulcerations, vasculitic rash, and upper andlower respiratory symptoms, including sinusitis and hemoptysis. • Although resolves after drug cessation,high-dose glucocorticoid or cyclophosphamide in severe cases • short-termhemodialysis
Iodine131 • preparations: sodium iodide 131 • MOA: trapped within the gland and enter intracellularly and delivers strong beta radiations destroying follicular cells • Clinical uses: Grave’s, primary inoperable thyroid CA • Contraindication: pregnancy
Iodine131 • Factors to attain adequate dose • maximum amount of radioactive iodine taken up by the gland • size and amount of tissue to be irradiated • effective half life of the isotope • relative sensitivity of the thyroid to the drug
Iodine131 • Thioamides should be given initially and stop 3 days before radioactive iodine administration • 131I dosage generally ranges between 185 MBq to 555 MBq repeated after 6 months • Adverse effects • permanent hypothyroidism • potential for genetic damage • may precipitate thyroid crisis
Anion Inhibitors • monovalent anions such as perchlorates, pertechnetate and thiocyanate can block uptake of iodide by the gland by competitive inhibition • can be overcome by large doses of iodides • useful for iodide-induced hyperthyroidism (amiodarone-induced hyperthyroidism) • rarely used due to its association with aplastic anemia
Inorganic Iodines • major anti-thyroids before the introduction of thioamides (1950s) • preparations: • strong iodine solution (Lugol’s) • potassium iodide • iodone
Inorganic Iodines • MOA: • acutely blocks release of thyroid hormone from the gland by inhibiting thyroglobulin proteolysis • inhibit iodide organification
Inorganic Iodines • Uses: • useful in thyroid storms: 2-7 days • iodides decrease vascularity, size and fragility of hyperplastic gland • Caution: • it may delay onset of thioamide effects; should be given after initiation of thioamides • The gland will escape from inhibition after 2-8 weeks.
Iodinated Contrast Media • iodinated contrast media – diatrizoate (oral) and iohexol (oral and intravenous) are valuable in hyperthyroidism (but is not labeled for this indication) • MOA: inhibits conversion of T4 to T3 in the liver, kidney, brain and pituitary; secondary MOA is due to inhibition of hormone release secondary to iodide levels in blood • useful in thyroid storms