Download
1 / 14
140 likes | 259 Views
Pectus Repair. Joseph Crossman. INTRODUCTION. Patient: N.A., 13 y/o male Focus: 1)To discuss history and assessment data 2)To identify nursing diagnoses and outline an appropriate plan of care. HEALTHY HISTORY. Brief History: Uncomplicated vaginal birth at term Pectus Excavatum

E N D
Pectus Repair Joseph Crossman
INTRODUCTION • Patient: N.A., 13 y/o male • Focus: • 1)To discuss history and assessment data • 2)To identify nursing diagnoses and outline an appropriate plan of care
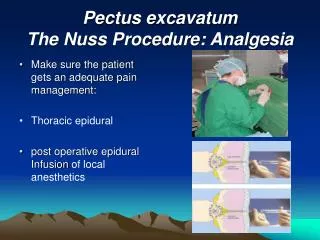
HEALTHY HISTORY • Brief History: • Uncomplicated vaginal birth at term • Pectus Excavatum • Asymptomatic until adolescent • Chief complaint = SOB • Nuss procedure
PSYCHOSOCIAL AND FAMILY HISTORY • Grandmother has custody • Mother and Father still together • Mother and Father still active in his life • Grandmother not at hospital • Cultural Considerations • Gamers, adolescent
CURRENT HOSPITALIZATION • Reason for Admit • Scheduled Nuss procedure • Primary complaint: Shortness of breath • Diagnosis: PectusExcavatum • Patho:congenital abnormal growth of the chest wall, characterized by an “inversion” of the chest • Treatment Plan:Surgery, PT, recovery
EXPECTED DEVELOPMENTAL STAGE • Theories: • Cognitive (Piaget): Formal Operations (Reasoning of abstract ideas) • Psychosocial (Erikson): Identity vs. Role Confusion (Finding “self”) • Psychosexual (Freud): Genital Stage (Strong interest in opposite sex) • IS THIS CHILD AGE APPROPRIATE? • Yes!
PHYSICAL ASSESSMENT • NEURO: Awake and alert x3. Fatigued. Reports nausea. Pain 0 at lowest 7 at highest • Respiratory: Crackles in lower quadrants, diminished sounds bilaterally. Saturation 88-94%. Weaning from 2L NC to RA (100% on 2L). RR 26. Cough on deep inspiration. • CV: No Exceptions. • GI: Hypoactive bowel sounds. Constipation – multiple urges with no movement.
PHYSICAL ASSESSMENT CON’T • GU: No exceptions. Voided at “last minute” of 1600 • SKIN:PIV @ L AC. Dressings at mid axillary line bilaterally at nipple height. • MUSCULOSKELETAL: Limited ROM in upper extremities. Lifting and ROM restriction – arms not allowed above or across chest. Severe pain/soreness along chest wall. • PSYCHOSOCIAL: Parents at bedside, active in care. • FALL RISK: Medium. Family constantly at bedside. Morphine PCA. Post-op.
Pt Initials: NA Age: 13 Medical Diagnoses: Pectis excavatum 1. Risk for Infection R/T: Surgery (Pectis repair) Temp: ↑39.2C WBC: 5.4k “Burning” pain at right sided surgical site. Meds: Cefazolin 5 Constipation R/t: medication side effects Patient’s urge, but inability to pass stools x4 during clinical day Hypoactive bowel sounds Pt report of nausea Morphine PCA, valium Meds: Colace, dulcolax 3. Acute pain R/T: Surgery Pt report of pain (4/10 resting) increasing during movement at surgical sites along chest wall. Meds: Morphine PCA Toradol 2. Impaired Gas exchange R/t: Anesthesia -O2 saturation falling to between 88-94% on RA -100% o2 sat with 2L/min NC -Dizziness with exercise -Morphine and valium ↓ respiratory effort 6 Psychosocial: Health seeking behaviors R/t: Increase in mobility with PT AEB: Patient states “I just want to move again even though it hurts” Patient asking when next PT session is Patient requesting to be OOB to chair 4. Impaired mobility R/t: dizziness, weakness, limitations of surgery -Dizziness with activity -Unsteady gait -Requires assistance with ambulation -Weakness with activity -May not use arms for support -Morphine, toradol, valium, Zofran, and dolcolax may all be contributing to dizziness
EXPECTED OUTCOMES • Risk for Infection: Temperature will remain below 38.5C during hospital stay, surgical sites will remain free of infection. • Impaired Gas Exchange: 02 Saturation on room air will stay above 95% throughout stay. • Acute pain: Pain scores will be 2/10 or below while resting during hospitalization, and remain so after discharge. • Impaired mobility: Patient will steadily increase his mobility and distance walked with PT daily. Patient will not experience a fall during hospitalization.
EXPECTED OUTCOMES 5. Constipation: Patient will be able to have a bowel movement P.O.D. 2. Patient will have regular bowel movements throughout hospital stay.
HOLISTIC CARE GIVEN • NURSING: • TRADITIONAL: • Incentive spirometer • VS q4h • Ambulation assistance • I&O • O2 2L/min NC (PRN) • D5 1/2NS with 20Meq KCL • Encouraged to void (techniques) • Pulse Oximetry • Patient/family teaching • COMPLIMENTARY/ALTERNATIVE: • Offer to perform healthcare activities for family • Offer refreshments or meals to family • Other family comfort measures • COLLABORATIVE: Physical therapy BID, regular diet, antibiotics (Vanco)
DISCHARGE PLANNING • Review S&S of infection • S&S of proper healing • Wound care basics • Provide information on resources to reduce caregiver role strain • Incentive Spirometer • Activity restrictions. NO LOG ROLLING/SIDE LAYING • Pain management • Alternate techniques • Side effects • Narcotics
RESEARCH • Implemented a respiratory care bundle to all patients post-op • Incentive spirometer x10/hour • Frequent oral care • Early ambulation/raised HOB • 6 Months before implementation, 33 patients were sent to ICU due to respiratory distress • 6 Months in the intervention, 15 were sent • 12 Months in the intervention, 6 were sent • Lamar, J. (2012). Relationship of respiratory care bundle with incentive spirometry to reduced pulmonary complications in a medical general practice unit.MEDSURG Nursing, 21(1), 33-37. Retrieved from http://ehis.ebscohost.com.proxy.lib.odu.edu/eds/detail?vid=10&sid=b8631269-3dcd-414c-9818- 91dba9ca5ea2@sessionmgr4002&hid=101&bdata=JnNpdGU9ZWRzLWxpdmUmc2NvcGU9c2l0ZQ==