Download
1 / 35
450 likes | 652 Views
Collaborative Atorvastatin Diabetes Study CARDS. Helen Colhoun, John Betteridge, Paul Durrington, Graham Hitman, Andrew Neil, Shona Livingstone, Margaret Thomason, Michael Mackness, Valentine Menys, John Fuller on behalf of the CARDS Investigators. CARDS The Rationale.

E N D
Collaborative Atorvastatin Diabetes StudyCARDS Helen Colhoun, John Betteridge, Paul Durrington, Graham Hitman, Andrew Neil, Shona Livingstone, Margaret Thomason, Michael Mackness, Valentine Menys, John Fuller on behalf of the CARDS Investigators
CARDSThe Rationale • Type 2 diabetes is associated with elevated cardiovascular risk • The role of lipid-lowering particularly with statins for secondary prevention of CHD is clear • More data on the benefits of lipid-lowering for the primary prevention of CHD and stroke are needed • The effectiveness and safety of lipid lowering for primary prevention in patients with low levels of LDL-C is unclear
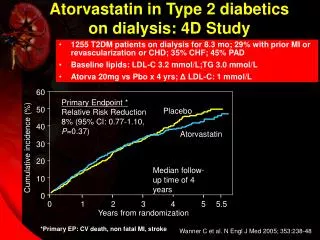
Aim of CARDS To evaluate the effectiveness and safety of atorvastatin 10mg daily versus placebo in the primary prevention of cardiovascular disease (major coronary events, revascularisation and stroke) in patients with type 2 diabetes without raised cholesterol levels
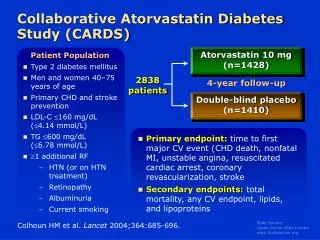
Placebo 2838 patients Atorvastatin 10mg CARDS Design Placebo 6 week pre-randomisation placebo run in phase then visits at month 1, 3, 6 and 6 monthly
CARDS Eligibility Criteria • Type 2 diabetes • Males or females • 40-75 years of age • No clinical history of coronary, cerebrovascular or severe peripheral vascular disease • LDL-C 4.14 mmol/L (160 mg/dL) • TG 6.78 mmol/L (600 mg/dL) • One of : • Hypertension defined as receiving antihypertensive treatment or SBP 140 mm Hg or DBP 90 mm Hg • Retinopathy • Microalbuminuria or macroalbuminuria • Current smoking
CARDS Endpoints Primary Efficacy Parameters • Acute CHD death • Non-fatal MI including silent MI • Hospitalised unstable angina • Resuscitated cardiac arrest • Coronary revascularisation • Stroke Major coronary events Secondary Efficacy Parameters • Total mortality • Any cardiovascular endpoint • Lipid and lipoproteins
CARDS Sample Size and Statistical Power Power 90% Significance level <0.05 Treatment effect 30% Assumed placebo event rate 2.35% per annum Sample size needed 2322 Allowing 20% dropout 2786 Randomised 2838 Expected termination 304 events – mid 2005 Actual termination after 2nd interim analysis 210 events – June 2003
CARDS Statistical Methods • Intention to treat analysis • Cox proportional hazards model of time to first primary end point (major coronary events and stroke) • Tested to show no treatment time interaction and the proportional hazard assumption holds • Main model then adjusted for age, sex, and stratified by centre • Tests for heterogeneity for subgroup analysis
Recruitment and Follow Up 4053 Screened 3249 (80%) Entered baseline 2838 (70%) Randomised 1428 Allocated atorvastatin 10mg daily 1410 Allocated placebo 1398 (99.1%) Complete follow up 1421 (99.5%) Complete follow up Lost to follow up for: mortality 4 (0.3%) morbidity 12 (0.9%)* Lost to follow up for: mortality 1 (0.1%) morbidity 7 (0.5%) * 1 subject lost after first primary endpoint
Follow up Time for Primary Endpoint Placebo Atorvastatin 10mg Median (min, max) 3.91 (1 day, 5.56yrs) 3.97 (1day, 5.51 yrs)
Placebo N (%) Atorvastatin N (%) Mean age (years) < 60 529 (37.5%) 558 (39.1%) 60-70 708 (50.2%) 703 (49.2%) > 70 173 (12.3%) 167 (11.7%) Women 453 (32.1%) 456 (31.9%) White ethnicity 1326 (94.0%) 1350 (94.5%) BMI Kg/m2 (SD) 28.8 (3.5) 28.7 (3.6) Obese (BMI >30Kg/m2) 537 (38.1%) 515 (36.1%) CARDS Patient Baseline Characteristics 61.8 61.5
CARDS Patient Baseline Characteristics PlaceboMean (SD)or N (%) AtorvastatinMean (SD)or N (%) Blood pressure Systolic BP (mmHg) 144 (16.1) 144 (15.9) Diastolic BP (mmHg) 83 (8.4) 83 (8.5) 940 (67) 956 (67) On BP drug Smoking 323 (22.9%) 308 (21.6%) Current Ex-smoker 601 (42.7%) 622 (43.6%) Never 485 (34.4%) 498 (34.9%)
PlaceboMean (SD) or N (%) AtorvastatinMean (SD) or N (%) Diabetes duration (years) 7.8 (6.3) 7.9 (6.4) Diabetes treatment Diet only 228 (16.2%) 214 (15.0%) Oral hypoglycaemic only 916 (65.0%) 932 (65.3%) Insulin only 207 (14.7%) 210 (14.7%) Insulin+oral hypoglycaemic 59 (4.2%) 72 (5.0%) HbA1c % 7.8 (1.4) 7.9 (1.4) Plasma glucose mmol/L 9.8 (3.2) 10.0 (3.3) CARDS Diabetes Related Characteristics
Clinical History* of Microvascular Disease Placebo N (%) Atorvastatin N (%) History of retinopathy 427 (30.3%) 426 (29.8%) Microalbuminuria (ACR >2.5mg/mmol) 153 (15.0 %) 148 (14.7 %) Macroalbuminuria (ACR >25 mg/mmol) 17 (1.7 %) 24 (2.4 %) Hypertension* 1184 (84.0 %) 1193 (83.5 %) *SBP≥140 mm Hg or DBP≥90 mm Hg or on BP drug
CARDS Patient Baseline Lipids* PlaceboMedian (IQR) AtorvastatinMedian (IQR) Total cholesterol (mmol/L) (mg/dL) 5.4 (4.8-5.9)207 (185-229) 5.4 (4.8-5.9)207 (186-228) LDL-cholesterol (mmol/L) (mg/dL) 3.1 (2.6-3.6)118 (100-137) 3.1 (2.6-3.6)119 (100-138) HDL-cholesterol (mmol/L) (mg/dL) 1.4 (1.2-1.6)53 (46-61) 1.3 (1.2-1.6)52 (45-60) * Subject to final verification
CARDS Patient Baseline Lipids* PlaceboMedian (IQR) AtorvastatinMedian (IQR) Triglycerides (mmol/L) (mg/dL) 1.7 (1.2-2.4)150 (106-212) 1.7 (1.2-2.4)150 (106-212) Non-HDL-C (mmol/L) (mg/dL) 3.9 (3.4-4.5)152 (130-174) 4.0 (3.4-4.5)154 (132-174) 150 (132-168) 115 (98-131) 150 (134-169) 116 (101-132) Apolipoprotein A1 (mg/dL) Apolipoprotein B (mg/dL) * Subject to final verificationIQR = Interquartile range
Compliance and Non-Study Statin Use % (n) Taking at least one statin by treatment arm* Year 1 Year 2 Year 3 Year 4 Average 9 Placebo 2.4 6.9 11.9 14.8 Atorvastatin 90.0 87.1 85.7 78.3 85.3 *% of those randomised and not known to be dead who have not yet had a primary endpoint at any given time. Assumes non-compliance if no compliance data available
Type of Event Placebo Atorvastatin 10mg No of events (% of patients with event) Any adverse event 13,365 (98%) 13,238 (97%) Associated AE 609 (25%) 599 (23%) Serious AE 920 (31%) 835 (29%) Associated SAE 20 (1.1%) 19 (1.1%) Discontinued for AE 145 (10%) 122 (8.5%) Adverse and Serious Adverse Events
Type of Event Placebo % of patients (n) Atorvastatin 10mg % of patients (n) Rhabdomyolysis 0% (0) 0% (0) CPK ≥ 10 ULN 1% (11) <1% (2) CPK ≥ 10 ULN & symptoms Myopathy AE report <1% (1) <1% (1) 0% (0) <1% (1) ALT ≥3 ULN 1% (14) 1% (17) AST ≥3 ULN <1% (4) <1% (6) Muscle and Liver Related Adverse Events
Specific Adverse Events Type of Event Placebo Atorvastatin 10mg Number of patients (% with event) Non CVD death* 48 (3.4 %) 41 (2.9%) 148 (10.5%) 15 (3.3%) 139 (9.7%) 16 (3.5%) Cancer or neoplasm Breast cancer or neoplasm 3 (0.2%) 4 (0.3%) Accident/suicide/violent death * Censoring time 3 weeks beyond last follow up date, not June 12th 2003
Lipid Levels by Treatment Total cholesterol (mmol/L) LDL cholesterol (mmol/L) Average difference 26% 1.4 mmol/L (54mg/dL) p<0.0001 Average difference 40% 1.2 mmol/L (46mg/dL) p<0.0001 6 4 3 4 2 2 1 0 0 0 1 2 3 4 4.5 0 1 2 3 4 4.5 Years of Study Years of Study Placebo Atorvastatin
Median Lipid Levels by Treatment Triglycerides (mmol/L) HDL cholesterol (mmol/L) Average difference 21% 0.4 mmol/L, 35mg/dL p=0<0.001 Average difference 1% 0.02 mmol/L, 0.8mg/dL p=0.4 1.4 2 1.2 1 .8 1 .6 .4 .2 0 0 0 1 2 3 4 4.5 0 1 2 3 4 4.5 Years of Study Years of Study Placebo Atorvastatin
Proportion Below LDL-C Guideline Target Levels (< 2.6 mmol/L or 100mg/dL) by Treatment
15 10 5 0 0 1 2 3 4 4.75 Cumulative Hazard for Primary Endpoint Relative Risk Reduction 37% (95% CI: 17-52) P=0.001 Placebo 127 events Cumulative Hazard (%) Atorvastatin 83 events Years Placebo 1410 1351 1306 1022 651 305 Atorva 1428 1392 1361 1074 694 328
Composition of Primary Endpointby Treatment Group Endpoint Category Placebo Atorvastatin 10mg Fatal MI 20 8 Other acute CHD death 4 10 Non fatal MI 41 25 Unstable angina 9 7 CABG or other surgery 18 12 Fatal stroke 5 1 Non fatal stroke 30 20 Total 127 83 *One atorvastatin group patient had a Non fatal MI followed by Surgery on the same day only the MI is shown One Placebo group patient had a CABG followed by stroke on the same day only the CABG is shown
Event Placebo* Atorva* Hazard Ratio Risk Reduction (CI) Primary endpoint 127 (9.0%) 83 (5.8%) 37% (17-52) p=0.001 Acute coronary events 77 (5.5%) 51 (3.6%) 36% (9-55) Coronary revascularisation 34 (2.4%) 24 (1.7%) 31% (-16-59) Stroke 39 (2.8%) 21 (1.5%) 48% (11-69) Treatment Effect on the Primary Endpoint .2 .4 .6 .8 1 1.2 Favours Atorvastatin Favours Placebo * N (% randomised)
Consistency of Effect No evidence of heterogeneity by: • Age p=0.58 • Sex p=0.59 • Baseline lipids p≥0.4 for all • Baseline systolic blood pressure p=0.2 • Retinopathy p=0.7 • Albuminuria p=0.34 • Smoking p=0.70
Treatment Effect onthe Primary Endpoint by Subgroup .2 .4 .6 .8 1 1.2 Favours Atorvastatin Favours Placebo * units in mmol/L (mg/dL) ** N (% of randomised)
Absolute Effect of Treatment PEP incidence rate / 100 person years at risk Placebo 2.46 Atorvastatin 1.54 Expected events per 1000 patients over four years Placebo 98.3 Atorvastatin 61.7 Events avoided per 1000 treated for four years 36.7 Absolute risk reduction in four years 3.7% NNT for four years 27
20 15 10 5 0 0 1 2 3 4 4.75 Cumulative Hazard for Any CVD Endpoint Relative Risk Reduction= 32% (95% CI 15-45) p=0.001 Placebo 189 events Atorvastatin 134 events Cumulative Hazard (%) Years Placebo 1410 1334 1275 992 621 287 Atorva 1428 1372 1337 1040 663 306
10 8 6 4 2 0 0 1 2 3 4 4.75 Cumulative Hazard for All Cause Mortality Relative Risk Reduction 27% (95%CI: -1-48) p=0.059 Placebo 82 deaths Cumulative Hazard (%) Atorvastatin 61 deaths Years Placebo 1410 1395 1370 1094 709 332 Atorva 1428 1418 1401 1110 730 351
Total deaths Coronary Other cardiac Cerebrovascular Other cardiovascular Total cardiovascular deaths Diabetes related death Cancer death Suicide accident or violent death Other death Total non-cardiovascular deaths Placebo 82 25 3 7 2 37 (2.6%) 1 30 3 11 45 (3.2 %) Atorvastatin 61 21 1 1 2 25 (1.8 %) 2 20 4 10 36 (2.5 %) Cause of Death By Treatment Arm
Summary • Trial terminated about 2 years earlier than anticipated, because a highly significant reduction in the PEP was observed at the 2nd interim analysis • 37% reduction in major CVD events • 48% reduction in stroke • 27% reduction in all cause mortality of borderline statistical significance • Consistent effect regardless of age, sex, lipids and complications (hypertension, smoking, retinopathy or macro/microalbuminuria) at baseline • Atorvastatin 10mg was well tolerated with no cases of rhabdomyolysis and no differences in muscle and liver adverse effects
Conclusion • CARDS shows that in patients with type 2 diabetes and with cholesterol levels at the lower end of the distribution, atorvastatin 10mg daily is safe and highly efficacious in reducing the risk of first CVD events, including stroke • CARDS suggests that there is no justification for having a threshold level of LDL-C as the sole arbiter of which patients with type 2 diabetes should receive statin treatment. The overall cardiovascular risk should be the principle determinant • The debate about whether all patients with type 2 diabetes warrant statin therapy should now focus on whether there are any patients at sufficiently low risk for this safe and efficacious treatment to be withheld