Download
1 / 45
450 likes | 959 Views
Vulvar cancer. ( 외음부암 ) 연세의대 산부인과학교실 김영태 교수. 학습목적 외음부에 생기는 악성종양들의 병리 , 증상 , 진단 및 치료 에 대한 지식을 습득하여 의심되는 병변에 대한 기본적 인 검사 및 상담을 할 수 있는 능력을 배양한다 . 학습목표 1. 외음부암의 증상 및 증세와 진단을 설명한다 . 2. 외음부암의 수술적 병기설정 (staging) 을 설명하고 예후 와 연관 짓는다 . 3. 외음부암의 수술적 치료와 방사선요법에 대하여 토론 한다 .

E N D
Vulvar cancer (외음부암) 연세의대 산부인과학교실 김영태 교수
학습목적 외음부에 생기는 악성종양들의 병리, 증상, 진단 및 치료 에 대한 지식을 습득하여 의심되는 병변에 대한 기본적 인 검사 및 상담을 할 수 있는 능력을 배양한다. 학습목표 1. 외음부암의 증상 및 증세와 진단을 설명한다. 2. 외음부암의 수술적 병기설정(staging)을 설명하고 예후 와 연관 짓는다. 3. 외음부암의 수술적 치료와 방사선요법에 대하여 토론 한다.
I. Introduction 1. Incidence ► About 4% of malignancies of the female genital tract ► Squamous cell ca : About 90% ► less common Melanomas Adenocarcinomas Basal cell ca Sarcoma ► The past two decades, In situ vulva cancer nearly doubled The rate of invasive squamous cell carcinoma has remained stable
2. Significant advances for management of vulvar cancer during the past 20 years ► Standard treatment : Radical vulvectomy en bloc groin dissection with or without pelvic lymphadenectomy ► Changes in management 1) Individualization of treatment 2) Vulvar conservation for unilateral vulvar cancer 3) Omission of the groin dissection for T1 tumors and ≤1mm of stromal invasion
4) Elimination of routine pelvic lymphadenectomy 5) The use ofseparate groin incision for the groin dissection to improve wound healing 6) Omission of the contralateral groin dissection in patients with lateral T1 lesions and negative ipsilateral nodes 7) The use of preoperative radiation therapy to obviate the need for exenteration in patients with advanced disease 8) The use of postoperative radiation to decrease the incidence of groin recurrence in patients with multiple positive groin nodes
II. Etiology 1. No specific etiologic factor 2. Risk factors ► Obese, hypertensive, diabetic or nulliparous women unable to confirm ► Common association between cervical, vaginal, and vulvar cancer suggests a common pathogen (Brinton et al.) ① Multiple sexual partners ② History of genital warts ③ Smoking
► HPV positive group : HPV positive 20 – 60% of patients with invasive vulvar cancer ► Occasionally associated with syphilis, nonluetic granulomatous venereal disease, particularly lymphogranuloma venereum, granuloma inguinale (donovanosis) *) 5% of vulvar cancer : positive serology test for syphilis
III. Invasive vulvar cancer **) Two different etiologic types of vulvar cancer 1. One type ① Young patients ② HPV infection related ③ Smoking ④ Commonly associated with basaloid or warty VIN 2. More common other types ① Elderly patients ② Unrelated to smoking or HPV infection ③ Concurrent VIN is uncommon ④ High incidence of dystrophic lesions including lichen sclerosus, adjacent to the tumor
**) Pathologic types of vulvar cancer 1. Squamous cell carcinoma( most common ) 2. Melanoma 3. Bartholin gland carcinoma 4. Other Adenocarcinomas 5. Basal cell carcinoma 6. Berrucous carcinoma 7. Vulvar Sarcomas 8. Rare Vulvar Malignancies 9. Secondary vulvar tumors
1. Squamous cell carcinoma ► Approximately 90~92% of all invasive vulvar cancers ► Mitoses ► Atypical keratinization - histologic hallmark of invasive vulvar cancer ► Anaplastic carcinoma : Consist of large immature cells spindle sarcomatoid cells or small cells
1) Microinvasive squamous cell carcinoma ① Definition Lesions ≤2cm with <1mm stromal invasion Depth of stromal invasion measured vertically from the most superficial basement membrane to the deepest tumor ② Metastasis to inguinal lymph nodes <1mm in depth or thickness : extremely rare >1mm : significant risk
2) Clinical features ► Predominantly a disease of postmenopausal women ► Mean age at diagnosis : about 65 years ■ Symptoms & Signs • Vulvar lump or mass • Long history of pruritus • Vulvar dystrophy • Vulvar bleeding • Discharge • Dysuria • Large metastatic mass in the groin, occasionally Less common
■ Physical examination • Lesion raised, freshly, ulcerated, leukoplakic, or warty in appearance • Labium majora most common site : labium minora, clitoris, perineum • Groin LN should be evaluated carefully • Complete pelvic exam should be performed • Pap smear, colposcopy of cervix and vagina should be performed
3) Diagnosis ► Wedge biopsy ► Excisional biopsy - if lesion < 1cm in diameter ►A common problem in the diagnosis of vulvar cancer : Physician’s delay, particularly if the lesions has a warty appearance 4) Routes of spread ① Direct extension to involve adjacent structures ② Lymphatic embolization to regional LN ③ Hematogenous spread to distant sites ( Lung, Liver, Bone, et. al.)
< Lymphatic metastasis > : Route : Inguinal LN Femoral LN Pelvic LN ( external iliac LN ) ■ Cloquet's node : Situated beneath the inguinal ligament The most cephalad of the femoral node group ■ Metastases to the femoral nodes without involvement of the inguinal nodes have been reported ■ Metastases to pelvic lymph nodes : about 9% About 20% of patients with positive groin nodes have positive pelvic lymph nodes
< Hematogenous metastasis > ■ Hematogenous spread usually occurs late in the course of vulvar cancer ■ It is rare in the absence of LN metastases 5) Staging ■ Clinical staging system based on the TNM classification adopted by FIGO in 1969 ■ When compared with surgical staging of vulvar Ca., the percentage of error in clinical staging increases from 18% for stage I disease to 44% for stage IV disease
외음부암의 병기체계(FIGO) 병기 TNM 정의 0기 Tis 상피내암 1기 T1N0M0 외음부 또는 회음부에 국한, 직경≤ 2cm, 림프절(-) 1a 간질 침윤 ≤1.0 mm 1b 간질 침윤 > 1.0 mm 2기 T2N0M0 외음부 또는 회음부에 국한, 직경>2cm, 림프절(-) 3기 T3N0M0 종양의 크기에 상관없이 T3N1M0 하부 요도 또는 항문 등 인접 장기로 파급, T1N1M0 편측 서혜부림프절 전이 T2N1M0 4기 4a T1N2M0 상부 요도, 방광 점막, 직장 점막, 골반 뼈 침범, T2N2M0 양측 서혜부림프절 전이 T3N3M0 T4anyNM0 4b anyTanyNM1 골반 림프절 전이를 포함한 원격 전이
6) Treatment ► En bloc radical vulvectomy and bilateral dissection of the groin and pelvic LNs : standard treatment ►Involving the anus, rectovaginal septum or proximal urethra, : occasionally was combined with the bone dissection ► Several factors led to modifications of standard Tx ① The disease is occurring in younger women, who are presenting with smaller tumors ② Concern about the postoperative morbidity, and associated long-term hospitalization after the en bloc radical dissection ③ Increasing awareness of the psychosexual consequences of radical vulvectomy
7) Management ■ Management of early vulvar cancer (T1N0-1) ► should be individualized ► Factors to consider in determining appropriate Tx ① The primary lesion ② the groin lymph nodes ► Management of primary lesion ①Radical vulvectomy vs. Radical local excision : incidence of local recurrence is not higher ②when combined with VIN, treatment is influenced by patient’s age ► Management of groin LNs ① With stromal invasion ≤1mm(no risk of LN mets) : groin dissection may be omitted. ② With stromal invasion >1mm : require inguinal-femoral lymphadenectomy
■ Management of T2, early T3 tumors and No-1 LNs ► Radical vulvectomy and bilateral inguinal - femoral lymphadenectomy ► Partial resection of organ if required ► Basic surgical approaches ① En bloc approach through trapezoid or butterfly incision ② Separate - incision approach ► One microscopically positive groin node no further therapy ►2 or more positive nodes groin irradiation
■ Complications of surgery ① Early complications ► Groin wound infection, necrosis and break down major immediate morbidity ► Urinary tract infection, seroma in femoral triangle, deep venous thrombosis, pulmonary embolism, myocardial infarction, hemorrhage and, rarely, osteitis pubis ► Anesthesia of the anterior thigh from femoral nerve injury
② Late complications ► Chronic leg edema major late complication ► Recurrent lymphangitis or cellulitis of legs ► Urinary stress incontinence, with or without genital prolapse ► Introital stenosis ► Femoral hernia ► Pelvic osteomyelitis ► Rectovaginal or rectoperineal fistula
■ Treatment of advanced disease ► Advanced disease (Def) : Large T3 or T4 primary tumor or the presence of bulky, positive groin nodes ► Should be individualized ► Pelvic exenteration combined with radical vulvectomy and bilateral groin dissection ► Radiation therapy ► Radiosurgical approach ► Chemoradiation ►Preoperative radiation with or without concurrent chemotherapy should be regarded as the treatment of first choice for advanced vulvar cancer patients
■ Current approach to pts with N2 or N3 groin LNs ► A preop C-T or Sono of pelvis to determine whether there are enlarged pelvic LNs ► All enlarged groin LNs are removed through a separate-incision approach and sent for frozen section diagnosis. If metastatic disease is confirmed, full lymphadenectomy is not performed ► Any enlarged pelvic nodes seen on CT or Sono are removed via an extraperitoneal approach. ► Full pelvic and groin irradiation. ► If the frozen section reveals no metastatic disease in the removed nodes, full groin dissection is performed.
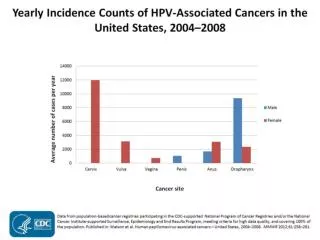
Locally advanced primary vulvar cancer Algorithm for the management of patients with locally advanced vulvar cancer CT scan of pelvis, abdomen and groin No suspicious nodes Suspicious nodes Bilateral inguinal-femoral lymphadenectomy Resect suspicious nodes and obtain frozen section Frozen section positive Frozen section negative Resect all bulky nodes from groin and pelvis Negative nodes 1-2 micrometastases Radiation therapy ± chemotherapy to vulva, groins and pelvis Radiation therapy ± chemotherapy to vulva • ≥ 3 micrometastases • Macrometastasis ≥ 10mm • Extracapsular speread Resect tumor bed (? biopsy only if complete clinical response)
■ Indications of radiotherapy ►Preoperatively, in patients with advanced disease who would require pelvic exenteration ►Postoperatively, to treat the pelvic lymph nodes and groin of patients with two or more positive groin nodes ■ Possible roles for radiation therapy ► Postoperatively, to prevent local recurrences in patients with involved or close margins(<5mm) ► As first therapy for pts with small primary tumor, particularly clitorial or periclitorial lesions in young and middle-aged women, due to significant psychological consequences
■ Recurrent vulvar cancer ► Correlates most closely with the number of positive groin nodes ► Positive LNs < 3 (microscopically involved) : a low incidence of recurrence at any site ► Positive LNs ≥ 3 : a high incidence of local, regional, and systemic recurrences ■ The most important independent prognostic parameters ① Lymph node involvement (P<0.0001) ② Tumor ploidy (p=0.0001) ③ Tumor size (p=0.0039)
2. Melanoma 1) Second most common vulvar malignancy 2) Predominantly in postmenopausal white women 3) Most commonly on the labia minor or clitoris 4) Symptoms & Signs No symptoms except for the presence of a pigmented lesion Itching or bleeding Groin mass (a few) 5) Histologic types a) superficial spreading melanoma b) Lentigo maligna melanoma c) Nodular melanoma : most aggressive 6) Staging : FIGO staging : not applicable
7) Treatment ► < 1mm of invasion : radical local excision alone ► ≥ 1mm of invasion : en bloc resection of the primary tumor and groin nodes ► Chemotherapy & immunotherapy : disappointing 8) Prognosis ► Overall prognosis : poor ► Mean 5 year survival rate : 21.7%-54% ► Corrected 5-year survival ( Chung et al. ) ≤ level II : 100% level III or IV : 40% level V : 20% ► Tumor volume ≤100mm3 : excellent prognosis
3. Bartholin gland carcinoma 1) About 5% of vulvar malignancies 2) Classification of a vulvar ca. as a Bartholin gl. Ca. ( Homan's criteria ) ① The tumor is in the correct anatomic position ② The tumor is located deep in the labium majors ③ The overlying skin is intact ④ There is some recognizable normal gland present
3) Treatment ① Traditional Tx : Radical vulvectomy, with bilateral groin and pelvic node dissection ② No indication for dissection of the pelvic nodes in the absence of positive groin nodes ③ Copeland et al. : Hemivulvectomy or radical local excision for the primary tumor ④ Preoperative radiation 4) Prognosis ① More advanced than squamous ca at the time of diagnosis, but the prognosis is similar
4. Other Adenocarcinomas 1) Usually arise in a Bartholin gland or occur in association with Paget's disease 2) Adenosquamous ca : particularly aggressive 3) Treatment : Radical vulvectomy, bilateral groin dissection and postop radiation
5. Basal cell carcinoma 1) About 2% of vulvar cancer 2) Most lesion are smaller than 2cm in diameter 3) Usually situated on the anterior labia majora 4) Usually affect postmenopausal white women and are locally aggressive 5) Radical local excision 6) Metastasis to regional lymph node : rare 7) Local recurrence rate : about 20% 8) Basosquamous ca : about 3-5% of basal cell carcinoma, Adenoid basal cell ca
6. Verrucous carcinoma 1) A variant of squamous cell carcinoma 2) Occur in postmenopausal women 3) Slowly growing but locally destructive lesions 4) Radical local excision-basic treatment 5) If the nodes + : Radical vulvectomy and bilateral inguinal-femoral lymphadenectomy are indicated 6) Radiation therapy is contraindicated, because it may induce anaplastic transformation with subsequent regional and distant metastases
7. Vulvar Sarcomas 1) 1-2% of vulvar malignancies 2) Constitute a heterogenous group of tumors 3) Leiomyosarcoma (most common), fibrosarcoma, neurofibrosarcoma, liposarcoma, rhabdomyosarcoma, angiosarcoma, epithelioid sarcoma, and malignant schwannoma 8. Rare Vulvar Malignancies 1) Lymphoma 2) Endodermal sinus tumor 3) Merkel cell ca. 4) Dermatofibrosarcoma protuberans 5) Malignant schwannoma
9. Secondary vulvar tumors 1) 8% of vulvar tumor-metastatic 2) Most common primary site-cervix followed by endometrium, kidney and urethra