Download

1 / 20
200 likes | 529 Views
The Increasing Use of Targeted Therapies for Leukemia and Lymphoma. Shira Dinner, MD Northwestern University. Educational Objectives. Define terminology used regarding leukemia Describe the latest developments in the treatment of acute lymphoblastic leukemia (ALL) Blinatumomab

E N D
The Increasing Use of Targeted Therapies for Leukemia and Lymphoma Shira Dinner, MD Northwestern University
Educational Objectives Define terminology used regarding leukemia Describe the latest developments in the treatment of acute lymphoblastic leukemia (ALL) Blinatumomab Inotuzumabozogamicin Chimeric antigen receptor T cells Engage patients and caregivers in clinical trial discussions on emerging therapies in ALL Identify strategies fro optimal patient care What is the best treatment for me?
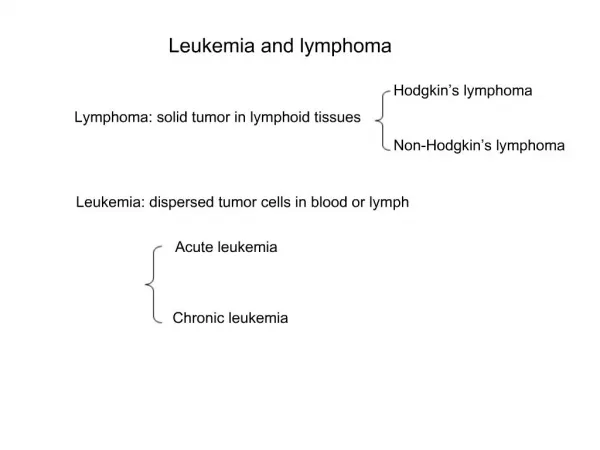
Common Terminology in Leukemia Acute: Develops from immature cells in the bone marrow that replicate quickly and aggressively The cells do not grow up and perform their normal function (i.e. fight infection) Chronic: Develops from mature cells that do not function normally Typically progresses more slowly Acute lymphoblastic leukemia: An aggressive cancer that develops from a type of white blood cells in the bone marrow called lymphocytes
Common Terminology in Leukemia Complete remission (CR) The absence of any signs or symptoms of the disease < 5% blast cells in the bone marrow (when looking at the cells under a microscope) and no evidence of leukemia anywhere outside of the bone marrow Minimal residual disease (MRD) A very low level of leukemia cells that remain in the bone marrow that cannot be seen by the microscope Detected by looking for certain gene or chromosome mutations that may be present in the leukemia or by looking at antigens (proteins) on the surface of the leukemia cells Refractory disease The leukemia does not respond to treatment or does not achieve a CR Relapsed disease The leukemia was in CR, but has now come back
Common Terminology in Leukemia Overall survival (OS) The length of time from either the date of diagnosis or the start of treatment for a disease that patients diagnosed are still alive. In a clinical trial, measuring the overall survival is one way to see how well a new treatment works. Progression free survival The length of time during and after the treatment of a diseasethat the disease remains in remission or does not get worse.
Immunotherapies Using the immune system to attack the leukemia • Antibody: A Y shaped protein made by the immune system to identify, bind, and neutralize harmful things (antigens) such as infections in the body • Immunotherapies: Use antibodies created in the lab to recognize and attack the leukemia cells
Antigens in ALL • There are many different proteins or antigens on the surface of ALL cells that we can design antibodies to target as part of immunotherapies
Phase 2 Blinatumomab in Relapsed/Refractory ALL 80% of patients had received at least 1 prior chemotherapy to treat relapsed or refractory ALL Topp et al. Lancet Oncology 2015;16(1):57-66.
Blinatumomab: Side effects • Most Common side effects • Fever 113 (60%) • Headache 65 (34%) • Neutropenic fever 53 (28%) • Neurologic side effects occurred in 98 (52%) patients, all reversible • This could include confusion or delirium to rarely stroke or seizure symptoms • Most were mild and resolved spontaneously74 (76%) • Most occurred during Cycle 1 85 (87%) • 29 pts discontinued for neuro side effects Topp et al. Lancet Oncology 2015;16(1):57-66. Topp et al. Lancet Oncology Jan;16(1):57-66.
Phase 3 IO vsStandard of Care (SOC) chemotherapy in relapsed/refractory ALL Safety The most common serious side effects were low blood counts Serious liver or gallbladder side effects occurred in 9% INO vs 3% SOC Veno-occlusive liver disease (VOD) 14% INO vs 1% SOC VOD: blockage in small veins in the liver that can cause fluid Retention and increased liver function tests (esp bilirubin) INO: 5 VOD events during treatment, 10 post SCT (2 fatal) DeAngelo et al. EHA 2015. Abstract 2073
IO Efficacy Treatment discontinuation: 83% INO mainly due to CR 89% SOC mainly due to resistant disease AlloHSCT 44% INO vs 18% SOC DeAngelo et al. EHA 2015. Abstract 2073
Generation of CAR T Cells ψ α-tumor scFv VL VH CD28 ζ chain 5’ LTR 3’ LTR ScFv SD SA T cell CD28 2. Subclone CAR gene into a vector CD19 1. Construct a CAR CD3ζ 3. Transduce and expand patient T cells ex vivo Retroviral vector encoding CD19 CAR cDNA CAR Tumor cell Genetically modified CD19-targeted T cell
Common Side Effects • Cytokine release syndrome (CRS) • Fever • Hypotension • Respiratory insufficiency • Neurological changes or symptoms • Delirium/disorientation • Global encephalopathy (tremors, seizure-like jerks) • Aphasia • Seizure • Can occur within 1-14 days of T cell infusion • Patients must be monitored in the hospital • More severe symptoms in patients with higher leukemia disease burden
Remaining questions with CAR T cells How long do CAR T cells last in the body? Do you need an allogeneic stem cell transplant after achieving remission with CAR T cells? Could patients be retreated with CAR T cells?
Possible side effects of CAR T cells Cytokine release syndrome Fever Neurotoxicity T-cell infusion reaction Tumor lysis syndrome Low B-cell levels (increased infection risk) GVHD The virus used to engineer the T cells could replicate in the patient’s body Uncontrolled T-cell proliferation The genetically modified product may insert itself into the patient’s DNA and cause other cancers Key toxicities observed in the Phase 1 studies Potential toxicities of CAR T cell therapy, but not observed in the Phase 1 studies
Summary New therapies for leukemia and lymphoma are taking advantage of copying or utilizing the immune system to attack the cancer Several new immunotherapies are available for ALL No clinical trials have compared blinatumomabvs IO vs CAR T cells We do not yet know which is the “best” treatment or what order we should give the treatments in It is important to consider side effects when selecting a treatment with your doctor Blinatumomab: neurologic side effects, cytokine release syndrome IO: liver side effects CAR T cells: CRS, neurologic side effects Talk to your doctor about a clinical trial