Download
1 / 39
390 likes | 508 Views
Screening for Co-occurring Disorder: Experience Implementing it in Multiple Regional Systems. Michael Dennis, Ph.D. Chestnut Health Systems, Normal, IL Barbara A. Lucenko, Ph.D. Research and Data Analysis Division of the Washington State Department of Social and Health Services, Olympia, WA

E N D
Screening for Co-occurring Disorder: Experience Implementing it inMultiple Regional Systems Michael Dennis, Ph.D. Chestnut Health Systems, Normal, IL Barbara A. Lucenko, Ph.D. Research and Data Analysis Division of the Washington State Department of Social and Health Services, Olympia, WA Ritchie Tidwell, MS. Tidwell and Associates, Columbia, SC Brian Rush, Ph.D. Centre for Addiction and Mental Health, Toronto, ON Presentation at the Joint Meeting on Adolescent Treatment Effectiveness (JMATE), Baltimore, MD, December 14–16, 2010.
Overview of the Global Appraisal of Individual NeedsShort Screener (GAIN-SS) Michael Dennis, Ph.D. Chestnut Health Systems, Normal, IL Presentation at the Joint Meeting on Adolescent Treatment Effectiveness (JMATE), Baltimore, MD, December 14–16, 2010. The presentation was supported with funds from the Center for Substance Abuse Treatment (CSAT), Substance Abuse and Mental Health Services Administration (SAMHSA) under contract 270-07-0191, as well as several individual CSAT, NIAAA, NIDA and private foundation grants. The opinions are those of the author and do not reflect official positions of the government. Available on line at www.chestnut.org/LI/Posters or by contacting Michael Dennis, Chestnut Health Systems, 448 Wylie Drive, Normal, IL 61761, phone 309-451-7801, fax 309-451-7765, e-Mail: mdennis@Chestnut.Org Questions about the GAIN can also be sent to gaininfo@chestnut.org
Provide an overview of the move towards screening brief intervention and referral to treatment Describe the Global Appraisal of Individual Needs Short Screener (GAINSS) and its use and validity for identifying co-occurring mental disorders, substance use disorders, and crime/violence Goals of This Presentation Are To…
Substance Use Disorders are Common, US Treatment Participation Rates Are Low Few Get Treatment: 1 in 19 adolescents, 1 in 21 young adults, 1 in 12 adults Over 88% of adolescent and young adult treatment and over 50% of adult treatment is publicly funded Much of the private funding is limited to 30 days or less and authorized day by day or week by week Source: OAS, 2009 – 2006, 2007, and 2008 NSDUH
The Movement to Increase Screening Screening, Brief Intervention, and Referral to Treatment (SBIRT) has been shown to be effective in identifying people not currently in treatment in several settings, initiating treatment/change, and improving outcomes (see http://sbirt.samhsa.gov/ ) The US Preventive Services Task Force (USPSTF; 2004, 2007), National Quality Forum (NQF, 2007), and Healthy People 2010 have each recommended: regular screening, brief intervention, and referral to treatment (SBIRT) for tobacco and alcohol abuse in general medical settings for everyone SBIRT for drug use in high-risk populations (e.g., adolescents, pregnant and postpartum women, people with HIV, and people with co-occurring psychiatric conditions) CSAT and NIDA are both funding several demonstration and research projects to develop and evaluate additional models for doing SBIRT in more settings/populations
Potential Screening/ Intervention Sites: Age 12 to 20 (38.1 million) Key potential of Workplace (e.g., EAP, Wellness,HRA) and School (e.g., SAP, EI, Prevention) Programs Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
The Global Appraisal of Individual Needs (GAIN) Is… A family of instruments ranging from screening to quick assessment to full biopsychosocial and monitoring tools Designed to integrate clinical and research assessment Designed to support clinical decision making at the individual client level across age & level of care Designed to support evaluation and planning at the program level Designed to support secondary analyses and comparisons across individuals and programs
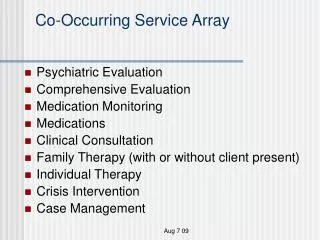
Gain Collaborators in the U.S. (August 2010) NH WA VT ME MT ND MA MN OR WI ID SD NY RI MI WY CT PA IA NV NE NJ OH UT IL IN CA DE CO WV VA MO MD KY KS DC NC TN OK NM State or Regional System GAIN Short Screener GAIN Quick GAIN Full No. of GAIN Sites AR AZ SC GA AL None (Yet) MS 1 to 14 TX LA FL 15 to 30 AK 31 to 165 HI More in BZ, CA, CN, JP, MX VI PR 3/10
Canada (August 2010) Number of GAIN Sites None (Yet) 1 to 14 15 to 30 31 to 165 Canada State or Regional System GAIN-Short Screener YT GAIN-Quick NU NT GAIN-Full NF BC AB MB QC SK PE ON NS NB
Some Numbers as of Summer 2010 1,501 licensed GAIN administrative units from 49 states (all but ND) and six countries 3,270 GAIN ABS users at 396 agencies 43,968 intake assessments (largest in field) 22,045 (88% with 1+ follow-up; largest follow-up data set in field) from 278 CSAT grantees 22 states, 12 federal agencies, six provinces, and three foundations mandate or strongly encourage its use Four dozen researchers have published 179 GAIN-related research publications to date Medicaid, Health Canada, several states, and private insurance systems accept it as evidence based
Across Measures, the GAIN Has a Common Factor Structure of Psychopathology * Symptoms of conduct disorder can also be caused by high levels of environmental crime and violence Source: Dennis, Chan, and Funk (2006) CFI = .92, RMSEA = .06 allowing for age
Co-Occurring Mental Health Problems Are Common, but the Type of Problems Also Changes with Age Internalizing disorders go up with age Externalizing disorders go down with age (but do NOT go away) Source: Chan, Y.-F., Dennis, M. L., & Funk, R. R. (2008). Prevalence and comorbidity of major internalizing and externalizing problems among adolescents and adults presenting to substance abuse treatment. Journal of Substance Abuse Treatment, 34(1) 14-24.
Progressive Continuum of Measurement (common measures) Screening to identify who needs to be assessed (5-10 min) Focus on brevity, simplicity for administration & scoring Needs to be adequate for triage and referral GAIN Short Screener for SUD, MH, and crime ASSIST, AUDIT, CAGE, CRAFT, DAST, MAST for SUD SCL, HSCL, BSI, CANS for mental health LSI, MAYSI, YLS for crime Quick assessment for targeted referral (20-30 min) Assessment of who needs a feedback, brief intervention, or referral for more specialized assessment or treatment Needs to be adequate for brief intervention GAIN Quick ADI, ASI, SASSI, T-ASI, MINI Comprehensive biopsychosocial (1–2 hours) Used to identify common problems and how they are interrelated Needs to be adequate for diagnosis, treatment planning, and placement of common problems GAIN Initial (Clinical Core and Full) CASI, A-CASI, MATE Specialized assessment (additional time per area) Additional assessment by a specialist (e.g., psychiatrist, MD, nurse, spec. ed.) may be needed to rule out a diagnosis or develop a treatment plan or individual education plan CIDI, DISC, KSADS, PDI, SCAN More Extensive / Longer / Expensive Screener Quick Comprehensive Special
GAIN Short Screener (GAIN-SS) • Administration Time: A 5-minute screener • Purpose: Used in general populations to • identify or rule out clients who will be identified as having any behavioral health disorders on the 60–120 min versions of the GAIN • triage area of problem • serve as a simple measure of change • ease administration and interpretation by staff with minimal training or direct supervision • Mode: Designed for self- or staff administration, with paper and pen, computer, on the web or in local IT application • Scales: Four screeners for Internalizing Disorders, Externalizing Disorders, Substance Disorders, and Crime/Violence Disorders, and a Total Disorder Screener
GAIN Short Screener (GAIN-SS) (continued) • Response Set: Recency of 20 problems rated past month (3), 2–12 months ago (2), more than a year ago (1), never (0)23 • Languages (23): American Sign Language, Arabic, Cambodian, English, Farsi, French, Hindi, Indonesian, Japanese, Korean , Laotian , Mandarin (simple & traditional), Marathi, Mongolian, Portuguese, Punjabi , Russian, Somali, Spanish (formal & informal), Tagalog, Vietnamese • Interpretation: Combined by cumulative time period as: • Past-month count (3s) to measure change • Past-year count (2s or 3s) to predict diagnosis • Lifetime count (1s, 2s, or 3s) as a measure of peak severity • Can be classified within time period as low (0), moderate (1–2), or high (3) • Can also be used to classify remission as early (lifetime but not past month) or sustained (lifetime but not past year) • Reports: Narrative, tabular, and graphical reports built into web- based GAIN ABS or ASP application for local hosting
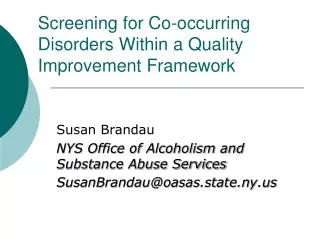
GAIN-SS Psychometric Properties Low Mod. High 100% Prevalence (% 1+ disorder) 90% Sensitivity (% w disorder above) 80% Specificity (% w/o disorder below) 70% (n = 6194 adolescents) 60% Using a higher cut point increases prevalence and specificity but decreases sensitivity 50% 40% At 3 or more symptoms we get 99% prevalence, 91% sensitivity, & 89% specificity 30% 20% 10% 0% 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Total Disorder Screener (TDScr) Total score has alpha of .85 and is correlated .94 with full GAIN version Source: Dennis et al., 2006
Moderate (1+) gives best result for sensitivity High (3+) gives best result for specificity GAIN-SS Performance by Subscale and Disorders Prevalence Sensitivity Specificity Screener/Disorder 1+ 3+ 1+ 3+ 1+ 3+ Internal Disorder Screener (0-5) Any Internal Disorder 81% 99% 94% 55% 71% 99% Major Depression 56% 87% 98% 72% 54% 94% Generalized Anxiety 32% 56% 100% 83% 44% 83% Suicide Ideation 24% 43% 100% 84% 41% 79% Mod/High Traumatic Stress 60% 82% 94% 60% 55% 90% External Disorder Screener (0-5) Any External Disorder 88% 97% 98% 67% 75% 96% AD, HD, or Both 65% 82% 99% 78% 51% 85% Conduct Disorder 78% 91% 98% 70% 62% 90% Substance Use Disorder Screener (0-5) Any Substance Disorder 96% 100% 96% 68% 73% 100% Dependence 65% 87% 100% 91% 30% 82% Abuse 30% 13% 89% 25% 14% 28% Recommend triage as 0 = Not likely 1-2 = Possible 3+ = Likely Crime/Violence Screener (0-5) Any Crime/Violence 88% 99% 94% 49% 76% 99% High Physical Conflict 31% 46% 100% 70% 38% 77% Mod/High General Crime 85% 100% 94% 51% 71% 100% Total Disorder Screener (0-5) Any Disorder 97% 99% 99% 91% 47% 89% Any Internal Disorder 58% 63% 100% 98% 8% 28% Any External Disorder 68% 75% 100% 99% 10% 37% Any Substance Disorder 89% 92% 99% 92% 20% 51% Any Crime/Violence 68% 73% 100% 96% 10% 32%
The Total Disorder Screener AlsoHelps to Predict Adolescent Level of Care About 30% of OP clients are in the high severity range more typical of residential Outpatient median = 6.0 (30% at 10+) Residential median = 10.5 (59% at 10+) (driven by comorbidity) Few missed (1/2 - 3%) Source: Dennis et al., 2006
Track gap between prior and current lifetime problems to identify “underreporting” Track progress in reducing current (past-month) symptoms) GAIN-SS Can Also Be Used for Monitoring 20 12+ Mon. ago (#1s) 2-12 Mon. ago (#2s) 16 Past Month (#3s) Lifetime (#1, 2, or 3) 11 12 10 10 9 9 8 8 3 4 2 2 0 Intake 3 6 9 12 15 18 21 24 Mon Mon Mon Mon Mon Mon Mon Mon Total Disorder Screener (TDScr) Monitor for relapse
GAIN Short Screener Profile: Reclaiming Futures (Range based on 0 / 1–2 / 3+ Symptoms) Source: Reclaiming Futures Portland, OR and Santa Cruz, CA sites (n = 192)
GAIN Short Screener Number of Problems Mod/Hi in Reclaiming Futures 93% endorsed one or more problems (40% four or more) Source: Reclaiming Futures Portland, OR and Santa Cruz, CA sites (n = 192)
Construct Validity of GAIN-SS Internalizing Disorder Screener Source: Education Service District 113 (n = 979) and King County (n = 1,002)
Construct Validity of GAIN-SS Externalizing Disorder Screener Source: Education Service District 113 (n = 979) and King County (n = 1002)
Construct Validity of GAIN-SS Substance Disorder Screener Source: Education Service District 113 (n = 979) and King County (n = 1002)
Construct Validity of GAIN-SS Crime/Violence Screener Source: Education Service District 113 (n = 979) and King County (n = 1002)
Other Validations Confirmatory Factor Analysis • Dennis, Chan, & Funk (2006) found that the 20-item GAIN-SS and its four subscales were highly correlated (.84 to .94) with the full scale, had 90% sensitivity and over 90% area under the curve relative to the full GAIN; confirmatory factors analysis also found it to be consistent with the overall model of psychopathology after allowing for age (CFI = .92; RMSEA = .06) Substance Disorders: • McDonnell and colleagues (2009) found that the 5-item GAIN-SS Substance Disorder Screener had 92% sensitivity and 85% correct classification relative to the Diagnostic Inventory Scale for Children (DISC) Predictive Scales (DPS; Lucas et al., 2001) and 88% sensitivity and 88% correct classification relative to the CRAFFT (Knight et al., 2001) Internalizing Disorders: • McDonnell and colleagues (2009) found that the 5-item GAIN-SS Internalizing Disorder Screener had 100% sensitivity and 75% correct classification relative to the Youth Self-Report (YSR; Achenbach et al., 2001) and that the 5-item GAIN-SS Externalizing Disorder Screener had 89% sensitivity and 65% correct classification to the YSR
Summary • The GAIN SS is a short efficient tool for identifying co-occurring disorders and grouping into one or more of four dimensions • It is correlated with several longer measures of substance use and other mental health issues • It is able to measure change and detect when someone is starting to lie • Having a common metric across the systems of care allow us to identify where people are coming into contact with the system and improve program planning • It was as or more sensitive than several clinical indicators
Identifying co-occurring disorders among social services clients in Washington State Barbara A. Lucenko, Ph.D. David Mancuso, Ph.D. Research and Data Analysis Division of the Washington State Department of Social and Health Services, Olympia, WA Michael Dennis, Ph.D. Chestnut Health Systems, Normal, IL Presentation at the Joint Meeting on Adolescent Treatment Effectiveness (JMATE), Baltimore, MD, December 14–16, 2010.
Background and Goals • In 2005 Washington State mandated the use of the GAIN Short Screen across all adolescent and adult chemical dependency, mental health, child welfare, justice and student assistance programs to have a common screener and metric • The goals of this presentation are to illustrate how this has been used by the state to • Understand the pattern of comorbidity across the service system • Validate the GAIN SS relative to clinical and administrative records • Guide program planning related to student assistance programs
Adolescent Rates of High (2+) Scores on Mental Health (MH) or Substance Abuse (SA) Screener by Setting in Washington State Problems could be easily identified Comorbidity is common Source: Lucenko et al. (2008). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Where in the System are the Adolescents with Mental Health, Substance Abuse and Co-occurring? There are more kids with mental health issues than substance use Source: Lucenko et al (2008). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Where in the System are the Adolescents with Mental Health, Substance Abuse and Co-occurring? 2/3rd of the teens with mental health issues are seen in substance abuse treatment or student assistance programs <1% <1% <1% student assistance programs Represent 1/3rd of the behavioral health system Source: Lucenko et al (2008). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Validation to Clinical Records • Mental health diagnoses recorded in medical records • Mental health and/or substance abuse treatment state service records • Arrests for substance-related crimes • Urine test results
Adolescent Client Validation of High Co-Occurring from GAIN Short Screener vs. Clinical Records by Setting in Washington State Two-page measure closely approximated prevalence found in the clinical record after the next 2 years Source: Lucenko et al. (2008). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
48% Both Significant Overlap (48%) in GAINSS and other Mental Health Indicators Among Youth in WA Chemical Dependence Programs 23% GAIN SS Only 12% Other Indicators Only Source: Lucenko et al. (2010). Co-occurring Mental Illness among Clients in Chemical Dependency Treatment. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1409/
Specificity for MH Disorder by Indicator among Youth in WA Chemical Dependency Programs Source: Lucenko et al. (2010). Co-occurring Mental Illness among Clients in Chemical Dependency Treatment. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1409/
Limitations • Report only represents adolescents who were screened in particular programs. There were kids not captured in these programs and other systems that were not included (e.g., Medicaid, developmental disabilities clients, other juvenile justice) • Validations compared multiple imperfect measures used in practice without any gold standard or formal resolution of when they did not agree • State used a binary (0–1 vs. 2–5) cut point instead of the trichotomy (0 vs. 1–2 vs. 3–5) recommended in the manual. While reasonable, this does impact some of the rates.
Summary • The GAIN SS was capable of efficiently identifying people with co-occurring disorders • Having a common metric across the systems of care allow us to identify where people are coming into contact with the system and improve program planning • It was as or more sensitive than several clinical indicators