Download
1 / 35
350 likes | 551 Views
Systemic and Pulmonary HTN in OSA. PAWAN CHAWLA, M.D. JNC 7. Express—Succinct evidence-based recommendations. Published in JAMA May 21, 2003, and as a Government Printing Office publication. Full Report—comprehensive justification and rationale (coming soon). HYPERTENSION.

E N D
Systemic and Pulmonary HTN in OSA PAWAN CHAWLA, M.D.
JNC 7 • Express—Succinct evidence-based recommendations. Published in JAMA May 21, 2003, and as a Government Printing Office publication. • Full Report—comprehensive justification and rationale (coming soon).
HYPERTENSION • HTN prevalence ~ 50 million people in the United States • The BP relationship to risk of CVD is continuous, consistent, and independent of other risk factors • Each increment of 20/10 mmHg doubles the risk of CVD across the entire BP range starting from 115/75 mmHg
Blood Pressure Classification 7Th Joint National Committee on High Blood Pressure
Benefits of Lowering BP 7Th Joint National Committee on High Blood Pressure
Benefits of Lowering BP In stage 1 HTN and additional CVD risk factors, achieving a sustained 12 mmHg reduction in SBP over 10 years will prevent 1 death for every 11 patients treated
Patient Evaluation • Evaluation of patients with documented HTN has three objectives: • Assess lifestyle and identify other CV risk factors or concomitant disorders that affects prognosis and guides treatment • Reveal identifiable causes of high BP • Assess the presence or absence of target organ damage and CVD
Identifiable Causes of Hypertension • Sleep apnea • Drug-induced or related causes • Chronic kidney disease • Primary aldosteronism • Renovascular disease • Chronic steroid therapy and Cushing’s syndrome • Pheochromocytoma • Coarctation of the aorta • Thyroid or parathyroid disease
WisconsinSleep Cohort Study Peppard et al: NEJM, 2000 A prospective, population-based study of the association betweenobjectively measured sleep-disordered breathing and hypertension Hypertension is defined as a laboratory-measured blood pressure of at least140/90 mm Hg or the use of antihypertensive medications. 709 subjects with follow up of 4 years Age 30 – 65 years
Sleep Heart Health Study Nieto et al: Jama, 2000 Cross-sectional analyses of participants in the Sleep Heart Health Study, a community-based multicenter study conducted between November 1995 and January 1998 6132 subjects Age 40 – 97 years
OSA & HTN • Gender Not Significant • Race Not Significant • Age Low risk Vs Not Significant • BMI Increased OR with decreasing BMI
UARS and Snoring and HTN • Young et al: Sleep, 1996 • Population-based sample of 580 adults was analyzed • Simple snoring represents the beginning of the SDB severity spectrum and that simple snoring has a proportionately smaller but, nevertheless, significant, risk for elevated blood pressure and CVD • Upper Airway Resistance Syndrome, Nocturnal Blood Pressure Monitoring, and Borderline Hypertension: Guilleminault et al: Chest, 1996 • Abnormalupper airway resistance during sleep, often associated withsnoring, can play a role in the development of hypertension
OSA/HTN + CPAP • Pepperell et al • 118 patients with ODI of 17/hr on cpap Vs subtherapeuticcpap(1cm) x 4weeks • Mean BP decreased by 2.4/3.4(sleep/wake) Vs an increase of 0.8 • Cpap > 5 hours needed
OSA/HTN + CPAP • Becker et al • 32 patients on cpap Vs subtherapeuticcpap(1cm) x 9 weeks • SBP/DBP decreased by 10 mm Vs no change • AHI decreased from 65 to 3 Vs 65 to 33
N=768 Becker et al: Circulation, 2003
Systolic HF & OSA • Prevalence of 5 – 32% • Sleep heart health study OR of 2.5 • Rx with cpap improves EF • EF predicts survival
Diastolic HF & OSA • OSA increase left ventricular mass left ventricular hypertrophy Diastolic dysfunction • Cpap improves Diastolic dysfunction
Bradyarrhythmias complete heart block, asystole • Ventricular arrhythmias • Atrial fibrillation increase recurrence rate
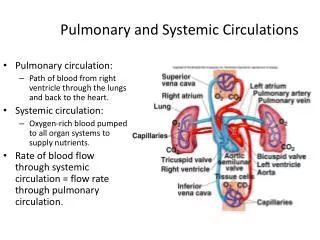
PHTN & OSA • Incidence 15-70% • Usually mild • Chaouat et al • 220 consecutive French patients with AHI > 20/hr • 17% had mean PAP >20 mm Hg • Patients with PAH had more severe OSA, higher Paco2 and BMI, lower Pao2, and more obstructive and restrictive defect • Paco2 and FEV1 were independent predictors of PAH
Laks et al • 100 consecutive Australian patients with AHI >20/hr • 42% had mean PAP > 20 mm Hg; range, 20 to 52 • Paco2, Pao2, and FEV1 accounted for 33% of variability in PAH • 6 patients with PAH had normal Pao2
Sanner et al • 92 consecutive German patients with OSA and AHI > 10/hr; range, 10-100/hr • COPD was an exclusion criterion • 20% had mild PAH; range, 20 to 25 mm Hg • 8 patients had increased PCWP; all had systemic hypertension • PCWP and time <90% saturation were independent predictors of PAH
Mechanism • Precapillary PAH • Hypoxemia • Hypercapnia • Changes in intrathoracic pressure • Endothelial dysfunction or remodeling • Capillary PAH • Loss of vascular surface area due to a cormorbid disorder, such as in COPD • Postcapillary PAH • LVH and diastolic dysfunction
Treatment • Motta et al • 6 patients, reduction of PAP with tracheostomy(45 to 22) • Alchanatis et al, Sforza et al, Sajkov et al • Reduction of PAP with cpap • Cpap required for > 5 hours