Download
1 / 7
90 likes | 287 Views
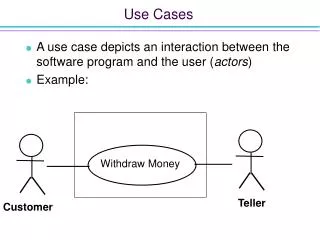
Use Cases. A Clinical outpatient facility providing images to a shared image repository. 2) Sending images and other clinical documents to a referring clinician without the use of CD media.

E N D
Use Cases A Clinical outpatient facility providing images to a shared image repository. 2) Sending images and other clinical documents to a referring clinician without the use of CD media. 3) Connecting a Hospital or Clinical practice PACS to a Regional Repository that is an XDS-I.b Image Document Source. 4) Submitting images for a clinical trial 5) Submitting Dose reports to a National registry.
A Clinical outpatient facility providing images to a shared image repository. Image Source Image Recipient shared Image repository Provide and Register Document Set-b [RAD-68] (Image Manager Instances Stored [RAD-70]) What would the number of Manifests to be included per transaction? (0-N?) 0-1 2) Special Metadata Considerations? Mandate metadata, if populated, needs to match images Patient ID must have the assigning authority , if affinity domain is known, must include Recipient may need to be an importer actor Accession number needs Issuer ID
Sending images and other clinical documents to a referring clinician (stand-alone) Image Source Image Recipient Provide and Register Document Set-b [RAD-68] 1) What would the number of Manifests to be included per transaction? (0-N?) 0-1 Special Metadata Considerations? None, manual lookup by patient name & demographics Does it make sense for multiple patient push? Probably not, use multiple submission sets/transactions) Note. Recipient is a drop box. Display is out of scope
Connecting a Hospital or Clinical practice PACS to a Regional Repository that is an XDS-I.b Image Document Source. Regional Repository Hospital Image Recipient XDS-I.b Image Document Source Image Manager/ Archive Image Source Provide and Register Document Set-b [RAD-68] (Image Manager Instances Stored [RAD-70]) What would the number of Manifests to be included per transaction? (0-N?) 0-1 A new manifest would have to constructed at the receiving end pointing to the receiving image document source for future retrieval transactions. No. Special Metadata Considerations? Mandate metadata, if populated by sender, needs to match images Patient ID must have the assigning authority , if affinity domain is known, must include Recipient may need to be an importer actor Accession number needs Issuer ID Associations linkages are out-of-scope
Submitting images for a clinical trial. Export Manager Image Source Image Recipient Receiver Provide and Register Document Set-b [RAD-68] (Export Instances [RAD-53] ) 1) What would the number of Manifests to be included per transaction? (0-N?) Special Metadata Considerations? Mandate metadata, if populated by sender, needs to match images Assigning authority may be specific to the clinical trial pseudononmynous namespace Patient ID must have the assigning authority , if affinity domain is known, must include Recipient may need to be an importer actor Accession number not important
Submitting Dose reports to a National registry. Dose Information Reporter Image Source Image Recipient Dose Registry Provide and Register Document Set-b [RAD-68] ([RAD-63] Submit Dose Information) 1) What would the number of Manifests to be included per transaction? (0-N?) - none Special Metadata Considerations? Assigning authority may be specific to the National Registry pseudo-anonymous namespace Patient ID must have the assigning authority , if affinity domain is known, must include Recipient may need to be an importer actor Accession number not important Consider limited Metadata Source Option
Need to consider groupings in general – examples: Importer actor could be considered as a minimum grouping for standalone . Source as an to an exporter/ media creator Using IOCM in XDR-I should be acceptable Do we need any special considerations for large image sets? Yes – a maximum buffer size needs to be defined for a transfer. Not a discoverable value. Recommend setting as 2GB. Need to review current XDR error states Does XOP cover compression or should we include zip as a package or other alternatives? Review in context to a generic XDR recipient. How do we handle association negotiation? We currently don’t. Is there any special considerations for a PHR? Metadata would not necessarily be equivalent with data transfer outbound. Bundling rules what has to, may and may not be permitted go together. Hasto (nothing) Should we include non-imaging objects? Yes. Report should be included in a submission set with the Image manifest, if possible. Use association link. Use manifest for the images when spanning multiple submission sets Review PDI in context to XDM for a possible XDM-I. Format code specification to include SOP class UID General considerations