Download
1 / 1
10 likes | 150 Views
A Pilot Study Investigating Older Women’s Health in Relation to Religiousness/Spirituality. Luciana Laganà, Giovanni Sosa, Luciana Esposito, Karine Mnatsakanyan, & Jennifer Wakefield California State University, Northridge - Department of Psychology

E N D
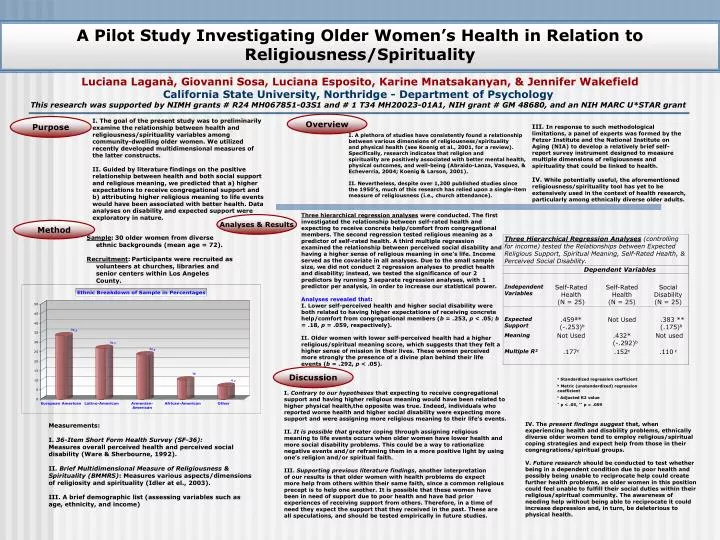
A Pilot Study Investigating Older Women’s Health in Relation to Religiousness/Spirituality Luciana Laganà, Giovanni Sosa, Luciana Esposito, Karine Mnatsakanyan, & Jennifer Wakefield California State University, Northridge - Department of Psychology This research was supported by NIMH grants # R24 MH067851-03S1 and # 1 T34 MH20023-01A1, NIH grant # GM 48680, and an NIH MARC U*STAR grant Overview Purpose I. The goal of the present study was to preliminarily examine the relationship between health and religiousness/spirituality variables among community-dwelling older women. We utilized recently developed multidimensional measures of the latter constructs. II. Guided by literature findings on the positive relationship between health and both social support and religious meaning, we predicted that a) higher expectations to receive congregational support and b) attributing higher religious meaning to life events would have been associated with better health. Data analyses on disability and expected support were exploratory in nature. III. In response to such methodological limitations, a panel of experts was formed by the Fetzer Institute and the National Institute on Aging (NIA) to develop a relatively brief self-report survey instrument designed to measure multiple dimensions of religiousness and spirituality that could be linked to health. IV. While potentially useful, the aforementioned religiousness/spirituality tool has yet to be extensively used in the context of health research, particularly among ethnically diverse older adults. I. A plethora of studies have consistently found a relationship between various dimensions of religiousness/spirituality and physical health (see Koenig et al., 2001, for a review). Specifically, research indicates that religion and spirituality are positively associated with better mental health, physical outcomes, and well-being (Abraido-Lanza, Vasquez, & Echeverria, 2004; Koenig & Larson, 2001). II. Nevertheless, despite over 1,200 published studies since the 1950’s, much of this research has relied upon a single-item measure of religiousness (i.e., church attendance). Three hierarchical regression analyses were conducted. The first investigated the relationship between self-rated health and expecting to receive concrete help/comfort from congregational members. The second regression tested religious meaning as a predictor of self-rated health. A third multiple regression examined the relationship between perceived social disability and having a higher sense of religious meaning in one’s life. Income served as the covariate in all analyses. Due to the small sample size, we did not conduct 2 regression analyses to predict health and disability; instead, we tested the significance of our 2 predictors by running 3 separate regression analyses, with 1 predictor per analysis, in order to increase our statistical power. Analyses revealed that: I. Lower self-perceived health and higher social disability were both related to having higher expectations of receiving concrete help/comfort from congregational members (b = .253, p < .05; b = .18, p = .059, respectively). II. Older women with lower self-perceived health had a higher religious/spiritual meaning score, which suggests that they felt a higher sense of mission in their lives. These women perceived more strongly the presence of a divine plan behind their life events (b = .292, p < .05). Analyses & Results Method Sample:30 older women from diverse ethnic backgrounds (mean age = 72). Recruitment:Participants were recruited as volunteers at churches, libraries and senior centers within Los Angeles County. Discussion a Standardized regression coefficient b Metric (unstandardized) regression coefficient c Adjusted R2 value * p < .05, ** p = .059 I. Contrary to our hypotheses that expecting to receive congregational support and having higher religious meaning would have been related to higher physical health,the opposite was true. Indeed, individuals who reported worse health and higher social disability were expecting more support and were assigning more religious meaning to their life’s events. II. It is possible that greater coping through assigning religious meaning to life events occurs when older women have lower health and more social disability problems. This could be a way to rationalize negative events and/or reframing them in a more positive light by using one’s religion and/or spiritual faith. III. Supporting previous literature findings, another interpretation of our results is that older women with health problems do expect more help from others within their same faith, since a common religious precept is to help one another. It is possible that these women have been in need of support due to poor health and have had prior experiences of receiving support from others. Therefore, in a time of need they expect the support that they received in the past. These are all speculations, and should be tested empirically in future studies. IV. The present findings suggest that, when experiencing health and disability problems, ethnically diverse older women tend to employ religious/spiritual coping strategies and expect help from those in their congregrations/spiritual groups. V. Future research should be conducted to test whether being in a dependent condition due to poor health and possibly being unable to reciprocate help could create further health problems, as older women in this position could feel unable to fulfill their social duties within their religious/spiritual community. The awareness of needing help without being able to reciprocate it could increase depression and, in turn, be deleterious to physical health. Measurements: I.36-Item Short Form Health Survey (SF-36): Measures overall perceived health and perceived social disability (Ware & Sherbourne, 1992). II. Brief Multidimensional Measure of Religiousness & Spirituality (BMMRS): Measures various aspects/dimensions of religiosity and spirituality (Idler at el., 2003). III. A brief demographic list (assessing variables such as age, ethnicity, and income)