Download
1 / 1
10 likes | 90 Views
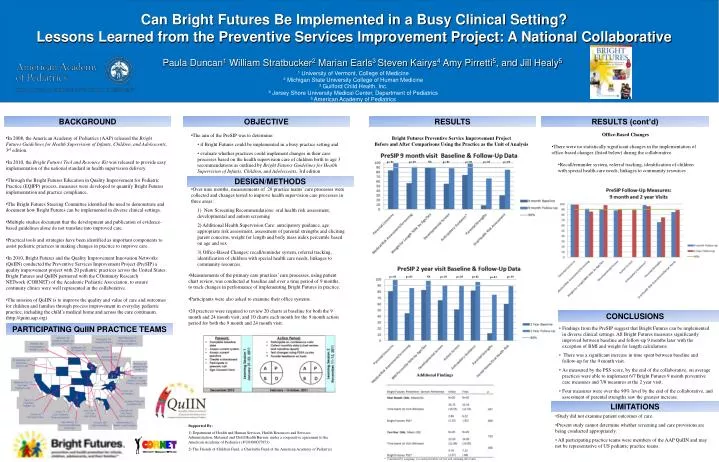
Can Bright Futures Be Implemented in a Busy Clinical Setting? Lessons Learned from the Preventive Services Improvement Project: A National Collaborative.

E N D
Can Bright Futures Be Implemented in a Busy Clinical Setting? Lessons Learned from the Preventive Services Improvement Project: A National Collaborative Paula Duncan1 William Stratbucker2 Marian Earls3 Steven Kairys4 Amy Pirretti5, and Jill Healy5 1 University of Vermont, College of Medicine 2 Michigan State University College of Human Medicine 3 Guilford Child Health, Inc. 4 Jersey Shore University Medical Center, Department of Pediatrics 5 American Academy of Pediatrics BACKGROUND OBJECTIVE RESULTS RESULTS (cont’d) • Office-Based Changes • There were no statistically significant changes in the implementation of office-based changes (listed below) during the collaborative. • Recall/reminder system, referral tracking, identification of children with special health care needs, linkages to community resources • The aim of the PreSIP was to determine: • if Bright Futures could be implemented in a busy practice setting and • evaluate whether practices could implement changes in their care processes based on the health supervision care of children birth to age 3 recommendations as outlined by Bright Futures Guidelines for Health Supervision of Infants, Children, and Adolescents, 3rd edition • Over nine months, measurements of 20 practice teams’ care processes were collected and changes tested to improve health supervision care processes in three areas: • 1) New Screening Recommendations: oral health risk assessment, developmental and autism screening • 2) Additional Health Supervision Care: anticipatory guidance, age appropriate risk assessment, assessment of parental strengths and eliciting parent concerns, weight for length and body mass index percentile based on age and sex • 3) Office-Based Changes: recall/reminder system, referral tracking, identification of children with special health care needs, linkages to community resources. • In 2008, the American Academy of Pediatrics (AAP) released the Bright Futures Guidelines for Health Supervision of Infants, Children, and Adolescents, 3rd edition. • In 2010, the Bright Futures Tool and Resource Kit was released to provide easy implementation of the national standard in health supervision delivery. • Through the Bright Futures Education in Quality Improvement for Pediatric Practice (EQIPP) process, measures were developed to quantify Bright Futures implementation and practice compliance. • The Bright Futures Steering Committee identified the need to demonstrate and document how Bright Futures can be implemented in diverse clinical settings. • Multiple studies document that the development and publication of evidence-based guidelines alone do not translate into improved care. • Practical tools and strategies have been identified as important components to assist pediatric practices in making changes in practice to improve care. • In 2010, Bright Futures and the Quality Improvement Innovation Networks (QuIIN) conducted the Preventive Services Improvement Project (PreSIP) a quality improvement project with 20 pediatric practices across the United States. Bright Futures and QuIIN partnered with the COntinuity Research NETwork (CORNET) of the Academic Pediatric Association, to ensure continuity clinics were well represented in the collaborative. • The mission of QuIIN is to improve the quality and value of care and outcomes for children and families through process improvement in everyday pediatric practice, including the child’s medical home and across the care continuum. (http://quiin.aap.org) Bright Futures Preventive Service Improvement Project Before and After Comparisons Using the Practice as the Unit of Analysis p<.01 p<.01 NS p<.01 p<.01 p<.01 p<.01 DESIGN/METHODS • Measurements of the primary care practices’ care processes, using patient chart review, was conducted at baseline and over a time period of 9 months, to track changes in performance of implementing Bright Futures in practice. • Participants were also asked to examine their office systems. • 20 practices were required to review 20 charts at baseline for both the 9 month and 24 month visit; and 10 charts each month for the 9 month action period for both the 9 month and 24 month visit. p<.01 p<.01 NS p<.01 p<.01 p<.02 p<.01 p<.01 CONCLUSIONS PARTICIPATING QuIIN PRACTICE TEAMS • Findings from the PreSIP suggest that Bright Futures can be implemented in diverse clinical settings. All Bright Futures measures significantly improved between baseline and follow-up 9 months later with the exception of BMI and weight for length calculations. • There was a significant increase in time spent between baseline and follow-up for the 9 month visit. • As measured by the PSS score, by the end of the collaborative, on average practices were able to implement 6/7 Bright Futures 9 month preventive care measures and 7/8 measures at the 2 year visit. • Four measures were over the 90% level by the end of the collaborative, and assessment of parental strengths saw the greatest increase. Additional Findings LIMITATIONS • Study did not examine patient outcomes of care. • Present study cannot determine whether screening and care provisions are being conducted appropriately. • All participating practice teams were members of the AAP QuIIN and may not be representative of US pediatric practice teams. Supported By: 1) Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau, under a cooperative agreement to the American Academy of Pediatrics (# U04MC07853) 2) The Friends of Children Fund, a Charitable Fund of the American Academy of Pediatrics * Calculated by assigning 1 to each preventive service and summing the results