Download
1 / 51
510 likes | 547 Views
Causes for primary immunodeficiencies. X linked agammaglobulinaemia X linked hypogammaglobulinaemia Immunoglobulin deficiency with increased IgM Immunoglobulin heavy chain gene deletion Kappa chain deficiency Common variable immunodeficiency IgA deficiency

E N D
Causes for primary immunodeficiencies X linked agammaglobulinaemia X linked hypogammaglobulinaemia Immunoglobulin deficiency with increased IgM Immunoglobulin heavy chain gene deletion Kappa chain deficiency Common variable immunodeficiency IgA deficiency Transient hypogammaglobulinaemia of infancy Selective IgG subclass deficiency
Combined immunodeficiency Severe combined immunodeficiency Adenosine deaminase deficiency Purine nucleoside deficiency Major histocompatibility complex (MHC)ii deficiency Reticular disgenesis
Hereditary Hemorrhagic Telangiectasia (Rendu-Osler-Weber Disease) - Autosomal dominant- tend to undergo repeated hemorrhage- Epistaxis may be an early sign- Pt. may suffer from anemia, but not usually life threatening.
Secondary Immunodeficiency Conditions · Infections HIV Acute severe viral infections Drug induced Immunosuppressive drugs Cytotoxic drugs Radiotherapy
Idiopathic Necrotizing Stomatitis • Consider: • Bacterial • Viral • Fungal • Combination Silverman, Eversole, Truelove. Essentials of Oral Medicine. London, B.C. Decker, 2001.
Minor Aphthous Ulcers Silverman, Eversole, Truelove. Essentials of Oral Medicine. London, B.C. Decker, 2001.
Myelo- or lymphoproliferativedisordes Myeloma Leukaemias Hodgkin’s and non Hodgkin’s lymphomas Metabolic disorders Malnutrition Iron deficiency Diabetes mellitus Autoimmune diseases SLE ITP Systemic scleroderma
Pernicious Anemia Pernicious anemia is a condition in which the body does not absorb vitamin B12. People who have this condition show signs of anemia, weakness, pallor, and fatigue on exertion. Other signs can include nausea, diarrhea, abdominal pain, and loss of appetite. The oral manifestations of pernicious anemia include angular cheilitis (ulceration and redness at the corners of the lips), mucosal ulceration, loss of papillae on the tongue, and a burning and painful tongue.
Iron deficiency. The tongue is devoid of filiform papillae. Angular cheilitis was also present in this patient.
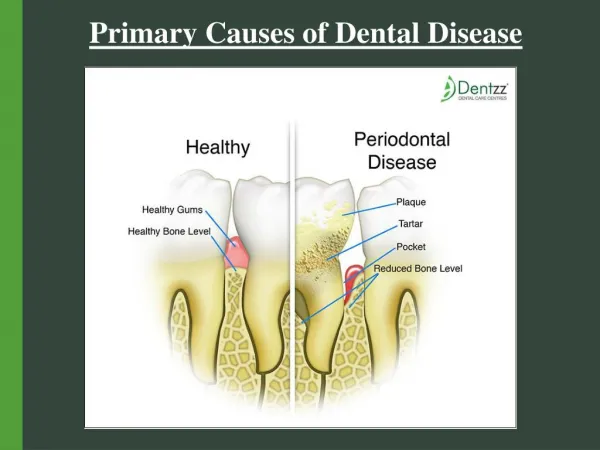
HIV-Associated Periodontitis • HIV-associated periodontis resembles acute necrotizing ulcerative gingivitis superimposed on rapidly progressive periodontitis. • Other symptoms include: • Interproximal necrosis and cratering • Marked swelling • Intense erythema over the free and attached gingiva • Intense pain • Spontaneous bleeding and bad breath
Atypical periodontal disease in a patient with HIV infection.
HIV Cervical Lymphadenopathy Enlargement of the cervical (neck) nodes. Lymphadenopathy is frequently seen in association with AIDS.
An immunologically mediated condition that presents in one of serval forms, and affects skin, CT and specific internal organs
Salivary Dysfunction & Xerostomia Salivary Hypofunction/ Dry mouth Dry mouth (xerostomia) occurs when the salivary glands are not functioning properly resulting in decreased saliva. Saliva not only aids in digestion, but is a necessary factor in oral health because it also helps to keep your mouth moist and prevent tooth decay. Diabetic neuropathy can also affect the salivary glands. Polyuria Topical treatments: fluoride containing mouthrinses salivary substitutes
Oral Candidiasis • Opportunistic fungal infection commonly associated with hyperglycemia. • Salivary dysfunction compromise immune function. • Salivary hyperglycemia provide substrate for fungal growth
Burning Mouth Syndrome Burning mouth syndrome is a condition with no determined cause and is characterized by a chronic burning pain in your mouth. This burning sensation can be severe, feeling much the same as scalding and can affect the overall areas of your mouth such as your tongue, gums, lips, inside of your cheeks, and the roof of your mouth. Although BMS has no known cause and finding treatment may by difficult, most people can bring it under control by working with an oral health specialist.
Oral manifestations of patients with hypothyroidism -delayed eruption, -enamel hypoplasia in both dentitions, -anterior open bite, -macroglossia, -micrognathia, -thick lips, -dysgeusia, -mouth breathing.
Oral manifestations of patients with hyperparathyroidism • 1. Dental abnormalities: -widened pulp chambers; -development defects; -alterations in dental eruption -weak teeth -maloclussions • 2. Brown tumor • 3. Loss of bone density • 4. Soft tissue calcifications
Oral manifestations of patients with hypoparathyroidism 1. Dental abnormalities: -enamel hypoplasia in horizontal lines; -poorly calcified dentin; -widened pulp chambers; -dental pulp calcifications; -shortened roots; -hypodontia; -delay or cessation of dental development. 2. Mandibular tori 3. Chronic candidiasis 4. Paresthesia of the tongue or lips 5. Alteration in facial muscles
Addison's disease Availability small (one to several square millimeters) grey-black spots or stripes, dark brown or grey-blue color without signs of inflammation on the mucous membrane of the: • mouth in the cheek area, • tongue edges, • palate, • gums. The spots can be oval or take the form of strips or fine grit, above the level of the mucous membrane, they are not separated.
Addison's disease The most common symptoms are fatigue, lightheadedness upon standing or while upright, muscle weakness, fever, weight loss, difficulty in standing up, anxiety, nausea, vomiting, diarrhea, headache, sweating, changes in mood and personality, joint and muscle pains.