Download
1 / 82
830 likes | 1.43k Views
Gas Exchange and Respiratory Function Part One. By Linda Self. Review of Terms. Cyanosis—influenced by polycythemia and anemia Clubbing- Schamroth method Hemoptysis Perfusion—actual blood flow through the circulation Ventilation----movement of gas into and out of the alveoli

E N D
Gas Exchange and Respiratory FunctionPart One • By Linda Self
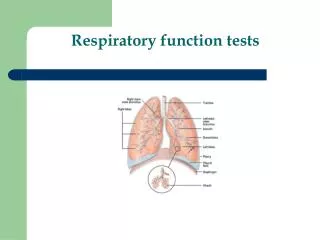
Review of Terms • Cyanosis—influenced by polycythemia and anemia • Clubbing-Schamroth method • Hemoptysis • Perfusion—actual blood flow through the circulation • Ventilation----movement of gas into and out of the alveoli • Diffusion—oxygen and CO2 exchanged from environment>trachea>bronchi>bronchioles and alveoli • Compliance-measure of the elasticity, expandability, and distensibility of lungs, influenced by surfactant
Ventilation—Perfusion Ratios • Normal lung is 1:1 • Shunts: when perfusionexceeds ventilation, a shunt exists. Blood bypasses the alveoli w/o gas exchange occurring. • Pneumonia, atelectasis, tumors, mucous plugs
Ventilation-Perfusion Ratios cont. • High ventilation-perfusion ratio---Deadspace • Ventilation exceeds perfusion • Alveoli do not have adequate blood supply for gas exchange to occur • Pulmonary emboli, pulmonary infarction, cardiogenic shock
Ventilation-Perfusion Ratios cont. • Silent unit—absence of ventilation and perfusion • Seen in pneumothorax and severe ARDS
Neurologic Control of Ventilation • Phrenic nerve • Respiratory center in medulla and pons • Central chemoreceptors in medulla, influenced by chemical changes in csf • Peripheral chemoreceptors in aortic arch and carotid arteries, respond first to changes in PaO2, then PaCO2 and pH
Gerontologic Considerations • Decreased strength of respiratory muscles • Decreased elasticity • Increased respiratory dead space • Decreased number of cilia • Decreased cough and gag reflex • Increased collagen of alveolar walls
Respiratory Assessment • Health History • Risk factors for respiratory disease-genetics, smoking, allergens, occupational and recreational exposure • Dyspnea, orthopnea • Cough, ?productive • Chest pain • Cyanosis • Lung sounds • Clubbing—indicates chronicity
Diagnostic Evaluation • PFTs-assess respiratory function, screening, assess response to therapy • FVC—vital capacity performed with a maximally forced expiratory effort • Forced expiratory volume—FEV1—volume of air exhaled in the specified time during the performance of forced vital capacity. FEV1 is volume exhaled in one second. • FEV1/FVC%--ratio of timed forced exp. volume to forced vital capacity
Diagnostic Evaluation--ABGs • 1. pH • 2. evaluate the PaCO2 and HCO3- • 3. Look to see if compensation has occurred. If CO2 is >40, respiratory acidosis; If HCO3- <24, metabolic acidosis; next look at value other than primary disorder, if moving in same direction as primary value, compensation is underway.
ABG’s continued • Can have two acid-base disturbances at same time • This can be identified when the pH does not explain one of the changes, e.g., • pH 7.2 • PaCO2 52 • HCO3 13 • Notice that oxygen level is not a component in determining the acid-base balance
ABGs cont. • Normal values for arterial gases: 7.35-7.45, CO2 35-45 mm Hg, HCO3 22-26 mEq/L, O2 80-100 mm Hg, BE +/-2 mEq/L sat >94% • Mixed Venous Blood: 7.33-7.41, CO2 41-51 mm Hg, HCO3 22-26 mEq/L, O2 35-40 mmHg, BE +/- 2mEq/L, sat 60-80% • See chapter 14 of text
Acidosis • Results in decreased myocardial contractility and a decreased vascular response to catecholamines. May interfere with metabolism of certain medications
Alkalosis • Can radically impair oxygen release from RBCs. For this reason, use bicarbonate infrequently in code situations
Other diagnostic studies • Pulse oximetry—not reliable in severe anemia, high CO levels, or in shock • CO2 monitoring—tells us ventilation to lungs is occurring, that CO2 is being transported to lungs, exp. CO2 indicates adequate ventilation • Cultures • Imaging—chest xray, CT, MRI, lung scans (inject isotope, inhale radioactive gas), PET • Bronchoscopy • Thoracentesis • others
Sleep Apnea • Associated with frequent, loud snoring with breathing cessation for 10 seconds or long, at least 5 episodes per hour, followed by awakening by a snort when O2 levels drop • May be associated with obesity • Decreased pharyngeal tone (related to alcohol, sedatives, neuromuscular disease)
Sleep Apnea • Diagnosed by polysomnography (ECG, EEG, EMG, pulse oximetry) • More common in men • High risk for CAD, cerebrovascular disease and premature death. • Results in hypoxia and hypercapnia which trigger sympathetic response. Can lead to dysrhythmias and elevated BP
Sleep Apnea signs and symptoms • Excessive daytime sleepiness • Frequent nocturnal awakening • Insomnia • Loud snoring • Morning headaches • Personality changes • Systemic hypertension • Dysrhythmias • Pulmonary hypertension, corpulmonale • polycythemia
Management • Nurse educates patient • Avoid alcohol and sedatives • Weight loss • CPAP or BiPAP—CPAP prevents airway collapse, BiPAP makes breathing easier and results in lower airway pressure • Uvulopalatopharyngoplasty • Tracheostomy • Provigil, Provera, Diamox, Triptil may help
Cancer of the Larynx • Squamous cell most common—95% • Increasing in women • More common in African Americans • Most common in individuals between 50-70 years of age • Carcinogens—tobacco, alcohol, exposure to asbestos, wood dust, cement dust, tar products, leather and metals • Most often affects glottic area
Laryngeal Cancer • Clinical manifestations • Hoarseness of greater than two weeks duration • Persistent cough • Sore throat • Dysphagia • Dyspnea • Ulceration • Foul breath • Cervical adenopathy • Weight loss • Debilitation
Assessment and Diagnosis • H&P • Laryngoscopy with biopsy/staging of disease • CT and MRI to assess adenopathy and further stageing
Laryngeal Cancer—Management • Depends on staging of tumor • Options include surgery, radiation and chemotherapy • Sometimes combination therapy • Ensure any dental problems corrected, usually before other treatments
Surgical Management • Laser surgery, supraglotticlaryngectomy, hemilaryngectomy, total laryngectomy • In case of total laryngectomy, advanced cancer present • Laryngeal structures removed including portion of trachea. Results in permanent loss of voice and permanent tracheostomy • Often will have radical neck dissection involves removal of sternocleidomastoid muscle, lymph nodes, jugular vein, surrounding soft tissue
Post-operative Care • Usually ICU postop • Monitor airway, VS, hemodynamic status and comfort level • Monitor for hemorrhage • Monitor for infection • Monitor tracheal stoma • Have extra trach at bedside (of same size!)
Post-operative Care • May be on ventilator initially • Will have trach • Ensure humidity at all times • May have split thickness skin graft or trapezius or pectoralis muscle grafts—ensure side of flap or graft not in dependent position • May have PCA • NG, G tube or jejunostomy tube may be in place—nutrition important • Speech rehab, esophageal speech, electrolarynges • Support group
Patients with chronic obstructive pulmonary disorders • COPD—nonreversible • Includes emphysema and chronic bronchitis • Can co-exist with asthma • Present with s/s in middle life and incidence increases with age • FVC and FEV1 decreased
Chronic Bronchitis • Disease of airways • Increased mucous production, decreased ciliary activity, inflammation, reduced alveolar macrophage function
Emphysema • Lobule—physiologic unit of lung consisting of bronchiole and its branches (alveolar ducts, sacs and alveoli) • Two types—panlobar and centrilobular • In Panlobartype—destruction of bronchiole, alveolar duct and alveoli; little inflammation, hyperexpanded chest, work on exhalation • Centrilobar type—derangement of the V/Q ratios, chronic hypoxemia, hypercapnea, polycythemia and right sided heart failure • See p. 688 for schematic
Emphysema • Risk factors include: • Cigarette smoking • Occupational dusts, chemicals, pollution • Deficiency of alpha1-antitrypsin, protective enzyme that protects lung parenchyma from injury---seen in Caucasians
COPD clinical manifestations • Chronic cough, sputum production, and dyspnea on exertion (DOE) • Weight loss common • Increased number of respiratory infections • In primary emphysema, will have “barrel chest”
Diagnosis of COPD • Thorough H&P • Spirometry to evaluate airflow obstruction • FEV1/FVC will be less than 70% • Reversibility will be tested • Chest xray • ABGs • Screening for alpha1-antitrypsin deficiency • Classified by five stages—0 through IV (see p. 690)
Medical Management • Smoking cessation will slow progression • May use Chantix, Wellbutrin, nortriptyline, clonidine • Bronchodilators—beta agonists, anticholinergics, methyxanthines, combinations, nebulized medications, inhaled and systemic corticosteroids • Influenza and pneumococcal vaccines • Oxygen therapy—usually started in severe COPD • High fat, low CHO diet
Oxygen Therapy in COPD • Previously felt that high levels of O2 affected hypoxic drive • Now thought that Haldane effect relates to ability of hgb to carry O2 and CO2. With increased levels of O2, increased saturation, increased CO2 load w/o being able to expel it. So, increased hypercapnia.
Surgical Management • Bullectomy—have blebs or enlarged airspaces that do not contribute to ventilation • Lung volume reduction surgery—may improve quality of life but not life expectancy • Lung transplantation
Nursing Management • Key is education • Breathing exercises • Inspiratory muscle training—breathe against a set resistance • Activity pacing • Self-care activities • Physical conditioning • Oxygen tx • Nutritional therapy • Coping measures
Bronchiectasis • Chronic, irreversible dilation of the bronchi and bronchioles • Caused by: inflammation d/t recurrent infections damaging bronchial walls, thick sputum and decreased mucociliary clearance; genetic disorders like CF, idiopathic causes • Results in atelectasis, fibrosis, VQ mismatch • R/O TB or other pathology • Tx-chest PT, smoking cessation, continuous abxtx, possible surgical resection of affected areas
Asthma • Chronic inflammatory disease characterized by mucosal edema, airway hyperreactivity, and mucous production • Largely reversible • Allergy is strongest predisposing factor • Poorly controlled asthma can result in remodeling. Bronchial muscles and mucous glands enlarge, alveoli hyperinflate and subbasement fibrosis.
Asthma • Cells that play role in inflammation of asthma include: leukotrienes, bradykinins, prostaglandins, mast cells, neutrophils, eosinophils • Beta receptor stimulation results in decrease of chemical mediators and causes bronchodilation • Three most common symptoms of asthma are cough, dyspneaand wheezing
Asthma • Family, environmental and occupational history is necessary • Comorbid conditions like GERD, drug-induced asthma and allergic bronchopulmonary aspergillosis may be present
Asthma • Triggers • Complications—status asthmaticus • Rescue and maintenance medications • Peak flow monitoring—measure highest airflow during a forced expiration. See asthma action plan on p. 715. Height, age and sex are variables to consider in personal best determination.
Status Asthmaticus • Severe and persistent asthma that does not respond to conventional therapy. Can be precipitated by infection, irritants, ASA or others • Severe bronchospasm with mucous plugging leading to asphyxia • Labored breathing, engorged neck veins, cough, wheezing • ABGs indicated • O2, IV fluids, burst of steroids, short acting corticosteroids, possibly magnesium sulfate • Nurse monitors, administers fluids and meds, ensures no irritants in environment
Atelectasis • Closure of collapse of alveoli • Often occurs in postoperative setting and in those who are immobilized • Can result from any obstruction that blocks air to and from alveoli
Atelectasis • Clinical manifestations—cough, sputum, low grade fever. In severe cases, tachycardia, tachypnea, central cyanosis • Chest xray may reveal patchy infiltrates, crackles will be heard over affected area, O2 saturation may be lower than 90%
Atelectasis • Prevention—turning, mobilizing patient, deep breathing maneuvers, incentive spirometry, secretion management such as suctioning, nebulizers, chest PT • Management—IPPB, chest PT, nebulizer tx, bronchoscopy, possible ventilator support, thoracentesis
Pneumonia • Is an inflammation of the lung parenchyma caused by microorganisms • Community acquired—usually caused by: Strep pneumo, Hemophilus influenza, Legionella, Mycoplasma pneumoniae, Chlamydia, viral • Hospital acquired—Pseudomonas, Staph aureus, Klebsiella
Pneumonia • Pneumonia in the immunocompromised patient—Aspergillus, Pneumocystis, Mycobacterium tuberculosis • Aspiration pneumonia • Is the most infectious disease causing death in the United States
Pathophysiology of pneumonia • Arises when normal flora has been aspirated, when host defenses are down or from bloodborne organisms that enter the pulmonary circulation • Affects ventilation and diffusion—will have adequate perfusion but not ventilation
Risk factors for Pneumonia • Conditions resulting in mucous obstruction (cancer, smoking, COPD) • Immunosuppression • Prolonged immobility • Depressed cough • NPO, ETT, NG or OG tubes • Alcohol intoxication • Advanced age • Medications that depress respirations
Clinical Manifestations of Pneumonia • Not possible to diagnose a certain type by manifestations alone • May be sudden in onset with fever, chills and pleuritic pain as seen in pneumococcal pneumonia • May be gradual in onset with low grade fever, HA, pleuritic pain, myalgias and pharyngitis • Orthopnea • Purulent sputum