Download
1 / 1
10 likes | 108 Views
No. 207. Outcomes of patients u ndergoing s urveillance for transitional c ell c arcinoma : Results from a Victorian tertiary h ospital. Nikhil Sapre, Paul Anderson, Anthony J. Costello, Christopher M. Hovens and Niall M. Corcoran

E N D
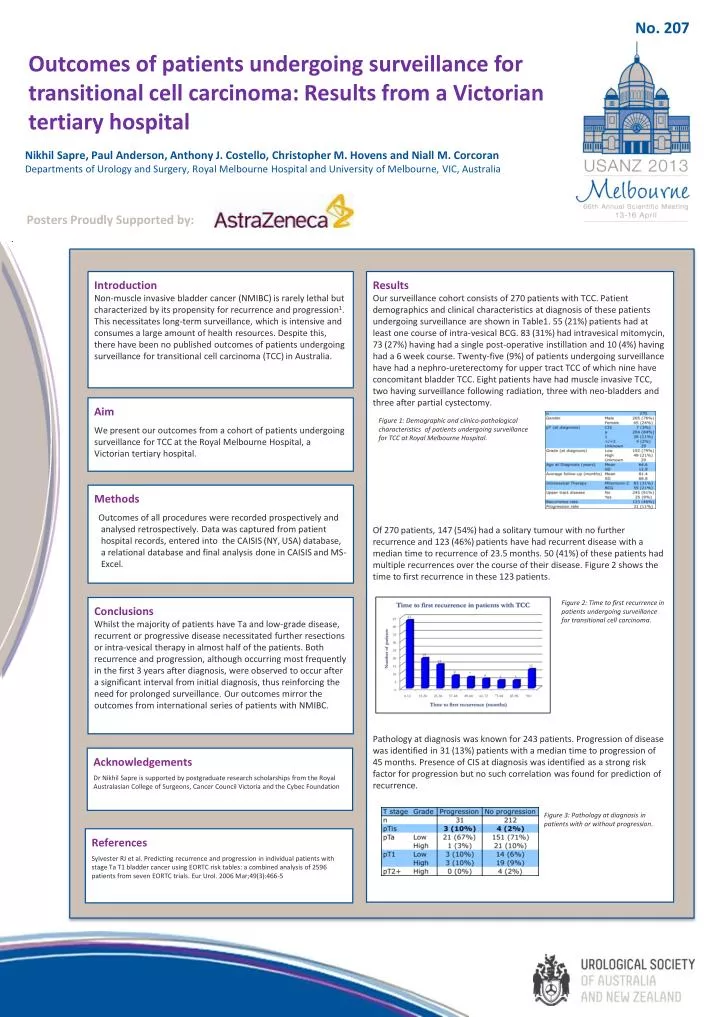
No. 207 Outcomes of patients undergoing surveillance for transitional cell carcinoma: Results from a Victorian tertiary hospital Nikhil Sapre, Paul Anderson, Anthony J. Costello, Christopher M. Hovens and Niall M. Corcoran Departments of Urology and Surgery, Royal Melbourne Hospital and University of Melbourne, VIC, Australia Posters Proudly Supported by: Results Our surveillance cohort consists of 270 patients with TCC. Patient demographics and clinical characteristics at diagnosis of these patients undergoing surveillance are shown in Table1. 55 (21%) patients had at least one course of intra-vesical BCG. 83 (31%) had intravesical mitomycin, 73 (27%) having had a single post-operative instillation and 10 (4%) having had a 6 week course. Twenty-five (9%) of patients undergoing surveillance have had a nephro-ureterectomy for upper tract TCC of which nine have concomitant bladder TCC. Eight patients have had muscle invasive TCC, two having surveillance following radiation, three with neo-bladders and three after partial cystectomy. Of 270 patients, 147 (54%) had a solitary tumour with no further recurrence and 123 (46%) patients have had recurrent disease with a median time to recurrence of 23.5 months. 50 (41%) of these patients had multiple recurrences over the course of their disease. Figure 2 shows the time to first recurrence in these 123 patients. Pathology at diagnosis was known for 243 patients. Progression of disease was identified in 31 (13%) patients with a median time to progression of 45 months. Presence of CIS at diagnosis was identified as a strong risk factor for progression but no such correlation was found for prediction of recurrence. Introduction Non-muscle invasive bladder cancer (NMIBC) is rarely lethal but characterized by its propensity for recurrence and progression1. This necessitates long-term surveillance, which is intensive and consumes a large amount of health resources. Despite this, there have been no published outcomes of patients undergoing surveillance for transitional cell carcinoma (TCC) in Australia. Aim We present our outcomes from a cohort of patients undergoing surveillance for TCC at the Royal Melbourne Hospital, a Victorian tertiary hospital. Figure 1: Demographic and clinico-pathological characteristics of patients undergoing surveillance for TCC at Royal Melbourne Hospital. Methods Outcomes of all procedures were recorded prospectively and analysed retrospectively. Data was captured from patient hospital records, entered into the CAISIS (NY, USA) database, a relational database and final analysis done in CAISIS and MS-Excel. Figure 2: Time to first recurrence in patients undergoing surveillance for transitional cell carcinoma. Conclusions Whilst the majority of patients have Ta and low-grade disease, recurrent or progressive disease necessitated further resections or intra-vesical therapy in almost half of the patients. Both recurrence and progression, although occurring most frequently in the first 3 years after diagnosis, were observed to occur after a significant interval from initial diagnosis, thus reinforcing the need for prolonged surveillance. Our outcomes mirror the outcomes from international series of patients with NMIBC. Acknowledgements Dr Nikhil Sapre is supported by postgraduate research scholarships from the Royal Australasian College of Surgeons, Cancer Council Victoria and the Cybec Foundation Figure 3: Pathology at diagnosis in patients with or without progression. References Sylvester RJ et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006 Mar;49(3):466-5






