Download
1 / 41
1.01k likes | 2.49k Views
Duloxetine in the Treatment of Diabetic Peripheral Neuropathic Pain (DPN). Contents. Introduction Mechanism of Action Efficacy in DPNP Pharmacokinetics, Safety and Tolerability Conclusion. Definition of diabetic neuropathy.

E N D
Duloxetine in the Treatment of Diabetic Peripheral Neuropathic Pain (DPN)
Contents • Introduction • Mechanism of Action • Efficacy in DPNP • Pharmacokinetics, Safety and Tolerability • Conclusion
Definition of diabeticneuropathy heterogeneous group of diseases that affect the autonomic and peripheral nervous systems of patients suffering from diabetes. WHO Definition: A disease characterized as a progressive loss of nerve fibers leading to sensation loss, foot ulceration, and amputation
Classification of Diabetic Neuropathy • Symmetric polyneuropathy • Autonomic neuropathy • Polyradiculopathy • Mononeuropathy
Multiple Mechanisms of Neuropathic Pain • Multiple mechanisms play a role in neuropathic pain: • Peripheral nervous system input: • Peripheral sensitization • Ectopic excitability • Central nervous system processing: • Central sensitization • Structural reorganization • Disinhibition 1. Woolf CJ. Ann Intern Med. 2004;140:441–451.
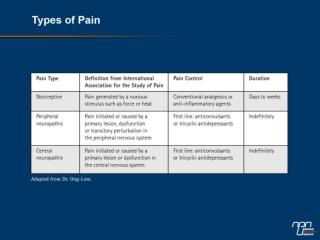
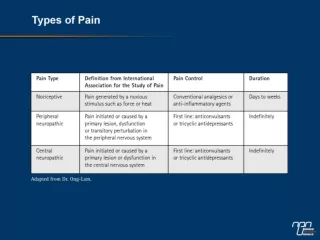
Nociceptive pain Adaptive Identifiable stimuli that normally produce tissue damage Usually self-limiting Transmitted by structurally and functionally intact pain pathways Examples: post-operative pain, burns, ischemic pain Neuropathic pain Maladaptive Often spontaneous (occurring without identifiable stimuli) Often chronic May involve structural and functional changes in pain pathways Examples: Polyneuropathy (eg, diabetic, HIV), trigeminal neuralgia, central post-stroke pain Distinguishing Nociceptive and Neuropathic Pain • Clinical pain syndromes occur along a spectrum from nociceptive to neuropathic • Nociceptive and neuropathic pain may coexist in the same patient 1. Portenoy RK and Kanner RM. Definition and assessment of pain. In: Portenoy RK and Kanner RM, eds. Pain Management: Theory and Practice;1996:4; 2. Galer BS and Dworkin RH. A Clinical Guide to Neuropathic Pain. Minneapolis: McGraw-Hill; 2000:8–9.
Evoked Pain hyperalgesia normal hyperpathia Magnitude of pain allodynia Stimulus intensity
Prevalence of Diabetic Neuropathyas a proportion of all diabetics 20 years after diagnosis
The majority of patients experience pain on a constant, daily basis1 DPNP Can Negatively Impact Patients’ Quality of Life1,2 “Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage3” mood sleep energy mobility work social activities enjoyment of life 1. Galer BS, et al. Diabetes Res ClinPract. 2000;47:123–128; 2. Benbow SJ, et al. QJM.1998;91:733–737;3. IASP website (http://www.iasp-pain.org/terms-p.html#Pain). Accessed October 05, 2006.
Goals of Neuropathic Pain Treatment • Primary goal = reduction in pain • Secondary goals • Improvement in physical function • Reduction in affective distress • Improvement in quality of life • Achieving these goals is predicated upon • Accurate diagnosis of any underlying etiology • Preventive treatment of underlying etiology (eg diabetes, joint inflammation, etc.), if possible 1. Turk DC. Clin J Pain. 2000;16:279–280; 2. Belgrade MJ. Postgrad Med. 1999;106:127–140.
Goals of Neuropathic Pain Treatment • Primary goal = reduction in pain • Secondary goals • Improvement in physical function • Reduction in affective distress • Improvement in quality of life • Achieving these goals is predicated upon • Accurate diagnosis of any underlying etiology • Preventive treatment of underlying etiology (eg diabetes, joint inflammation, etc.), if possible 1. Turk DC. Clin J Pain. 2000;16:279–280; 2. Belgrade MJ. Postgrad Med. 1999;106:127–140.
Management of DPNP • Off-Label Agents:1 • Tricyclic antidepressants – i.e., amitriptyline • Anticonvulsants – i.e., gabapentin • Opioid analgesics • Tramadol • Other antidepressants – i.e., venlafaxine • FDA-Approved Agents in US: • Cymbalta2 • Lyrica3 1. Argoff CE, et al. Mayo Clin Proc. 2006;81(4):S12–25; 2. Cymbalta US Prescribing Information; 3. Lyrica US Prescribing Information.
Contents • Introduction • Mechanism of Action • Efficacy in DPNP • Pharmacokinetics, Safety and Tolerability • Conclusion
Nerve lesion Ectopic discharges Ectopic discharges Nerve lesion induces hyperactivity due to changes in ion channel function Perceived pain Descendingmodulation Ascendinginput Nociceptive afferent fiber Spinal cord Adapted from Doubell et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed. 1999.;165-182
Noxiousstimuli Loss of inhibitory controls Loss of descending modulation causes exaggerated pain due to an imbalance between ascending and descending signals Exaggerated painperception Loss ofdescendingmodulation Ascendinginput Nociceptive afferent fiber Spinal cord Adapted from Doubell et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed. 1999.;165-182 Attal N et al. Acta Neurol Scand. 1999;173:12-24. Woolf CJ et al. Lancet. 1999;353:1959-1964. Roberts et al. In Casey KL (Ed). Pain and central nervous system disease. 1991
Abnormal discharges induce central sensitization Tactilestimuli Intact tactile fiber Central sensitization After nerve injury, increased input to the dorsal horn can induce central sensitization Perceived pain Nerve lesion Descendingmodulation Ascendinginput Nociceptive afferent fiber Perceived pain(allodynia) Descendingmodulation Ascendinginput Adapted from Doubell et al. in Wall PD, Melzack R (Eds). Textbook of pain. 4th Ed. 1999.;165-182
Serotonin & Norepinephrine Play a Major Role in Pain • Neuropathic pain is associated with increased excitation and decreased inhibition of ascending pain pathways • Descending pathways modulate ascending signals • NE and 5-HT are key neurotransmitters in descending inhibitory pain pathways • Increasing the availability of NE and 5-HT may promote pain inhibition centrally 5-HT NE 1. Figure adapted from: Fields HL and Basbaum AI. Central nervous system mechanisms of pain modulation. In: Wall PD and Melzack R, eds. Textbook of Pain, 4th ed. Churchill Livingstone: London, UK;1999,310.
The Combination of an NRI and an SSRI is More Effective than Either Alone Total paw-licking time (late phase) 120 Paroxetine Vehicle control 100 Thionisoxetine 80 Paroxetine 1 mg/kg + Thionisoxetine Less Pain Behavior % of Vehicle Control * * 60 40 N=5–12 * P < .05 20 vs thionisoxetine alone 0 0.1 1 10 Drug (mg/kg) Higher Dose 1. Iyengar S, et al. J Pharmacol Exp Ther. 2004;311:576–584.
Less Pain Behavior % of Vehicle Control Drug (mg/kg i.p. 30 min) Drug (mg/kg i.p. 30 min) Higher Dose Higher Dose Duloxetine Venlafaxine Milnacipran Amitriptyline Duloxetine is a Potent Inhibitor of Persistent Pain in the Formalin Model Total paw-licking time (late phase) Vehicle control Vehicle control 100 100 * 75 75 * * * * * 50 50 * * * # * 25 25 * * 0 0 1 10 100 1 10 100 N=6–9 * P < .05 vs vehicle # Rotorod effects 1. Iyengar S, et al. J Pharmacol Exp Ther. 2004;311:576–584.
Duloxetine Reverses Mechanical Allodynia in the Spinal L5/L6 Nerve Ligation Model of Neuropathic Pain 14 * Vehicle control 12 Duloxetine 30 mg/kg p.o. once daily 10 8 Less Pain Behavior Withdrawal Threshold Response (g) N=4–5 6 4 * P < .05 vs vehicle 2 0 pre base Day 1 3 hrs Time pre = pre-surgery baseline, base = post-surgery baseline 1. Iyengar S, et al. J Pharmacol Exp Ther. 2004;311:576–584.
Contents • Introduction • Mechanism of Action • Efficacy in DPNP • Pharmacokinetics, Safety and Tolerability • Conclusion
Completed Duloxetine Clinical Trials in DPNP 1. Goldstein DJ, et al. Pain. 2005;116:109–118; 2. Wernicke JF, et al. Neurology. 2006;67:1411–1420; 3.Raskin J, et al. Pain Med. 2005;6:346–356; 4. Data on file, Eli Lilly; 5. Poster: Raskin J, et al. 25th American Pain Society (APS) Annual Scientific Meeting; San Antonio, TX; May 3–6, 2006;6. Raskin J, et al. Pain Med. 2006;7:373–385.
Duloxetine Reduces 24-Hour Average Pain Severity in DPNP Pooled data from 3 studies 0.0 Placebo(n=330) Duloxetine20 mg QD(n=111) Duloxetine60 mg QD(n=334) Duloxetine60 mg BID(n=333) -0.5 * -1.0 Mean Change in 24-hourAverage Pain Severity Score -1.5 * * Improvement * -2.0 * * * * * * * * * -2.5 * * * * * * -3.0 * * * * * * P ≤ .05 -3.5 0 1 2 3 4 5 6 7 8 9 10 11 12 13 vs placebo Weeks MMRM • A reduction of approximately 2 points or 30% represents a clinically important difference (mean baseline score was 5.83) Poster: Raskin J, et al. 25th American Pain Society (APS) Annual Scientific Meeting; San Antonio, TX; May 3–6, 2006.
*** *** ** ** ** ** PlaceboDuloxetine 20 mg QDDuloxetine 60 mg QDDuloxetine 60 mg BID Duloxetine Improves Response Rates in DPNP After 12 Weeks† 30% Reduction in 24-hour Average Pain 50% Reduction in 24-hour Average Pain *** *** *** ** * * Study 11 Study 23 Study 31 Study 12 Study 23 Study 34 * P < .05vs placebo ** P < .01vs placebo *** P < .001vs placebo † Completer analysis 1. Presentation: Raskin J, et al. 41st European Association for the Study of Diabetes (EASD) Annual Meeting; Athens, Greece; September 12–15, 2005; 2. Goldstein DJ, et al. Pain. 2005;116:109–118; 3. Wernicke JF, et al. Neurology. 2006;67:1411–1420; 4. Raskin J, et al. Pain Med. 2005;6:346–356
60 mg QD Duloxetine Improves Worst Pain Severity in DPNP Data from three 12-week efficacy and safety studies 1 2 3 n=112 n=110 n=114 n=111 n=106 n=103 Placebo Duloxetine 60 mg QD ** ** * * P ≤ .05, ** P < .001 MMRM 1. Goldstein DJ, et al. Pain. 2005;116:109–118; 2. Wernicke JF, et al. Neurology. 2006;67:1411–1420; 3.Raskin J, et al. J Pain Med. 2005;6:346–356.
60 mg QD Duloxetine Reduces Pain at Night in DPNP Data from three 12-week efficacy and safety studies 1 2 3 n=111 n=112 n=106 n=109 n=103 n=114 Placebo Duloxetine 60 mg QD ** * ** * P ≤ .05, ** P < .05 1. Goldstein DJ, et al. Pain. 2005;116:109–118; 2. Wernicke JF, et al. Neurology. 2006;67:1411–1420; 3.Raskin J, et al. JPain Med. 2005;6:346–356.
Do Improvements in Pain Ratings Correspond to Patients Actually Feeling Better? • In clinical trials, efficacy is often measured with numerical or categorical pain scales • Scales used in the Cymbalta DPNP clinical trials include • 24-hour Average Pain Likert Scores • Brief Pain Inventory (BPI) Average Pain Score1 Pain as bad as you can imagine Please rate your pain by circling the one number that best describes your pain on average NoPain 0 1 2 3 4 5 6 7 8 9 10 • Global assessment of improvement assessed in Cymbalta DPNP Clinical Trials: Patient Global Impression of Improvement (PGI-I) Scale2 Check one box that best describes how you have felt overall since you began taking this medication 1 Very much better 3 A little better 5 A little worse 2 Much better 4 No change 6 Much worse 7 Very much worse 1. Cleeland CS and Ryan KM. Ann Acad Med Singapore. 1994;23:129–138; 2. Guy W. ECDEU Assessment Manual for Psychopharmacology. 1976;217–222:313–331.
0 -0.5 -1 -1.5 -2 -2.5 -3 -3.5 PlaceboDuloxetine 60 mg QDDuloxetine 60 mg BID Duloxetine Decreased the Impact of Pain on Daily Activity, Function, and Enjoyment of Life (BPI-I) Pooled data from 3 studies Enjoyment of Life BPI Avg Score Walking Ability Normal Work Relationship With Others General Activity Sleep Mood LS Mean Change from Baseline BPI-I Score * Decreased Impact / Improvement *** *** *** *** ** *** *** *** *** *** *** *** *** ** *** * P < .05 vs placebo ** P < .01 vs placebo *** P < .001 vs placebo Armstrong DG, et al. Pain Med. 2007;8(5):410-418.
PGI-Improvement at Endpoint of Maintenance Phase Improvement Responders (60 mg) Non-Responders (120 mg) Responders defined as ≥30% reduction on BPI average pain during acute phase. PGI-Improvement = Patient’s Global Impression of Improvement Data on File
Contents • Introduction • Mechanism of Action • Efficacy in DPNP • Pharmacokinetics, Safety and Tolerability • Conclusion
Duloxetine Pharmacokinetic Data • Clinical pharmacology1-7: • t1/2 about 12 hours (in plasma) • Protein binding >90% • Observed duration of action with once-daily dosing suggests: • Therapeutic effects may persist after drug is cleared • Brain concentration may differ from plasma concentration • No need for dose adjustment based on • Age, gender and/or smoking • Excretion data 1. Sharma A, et al. J Clin Pharmacol. 2000;40:161–167; 2. Skinner MH, et al. Clin Pharmacol Ther. 2000;67:129; 3. Takahashi A, et al. Neuropsychopharmacology. 1994;10 (Supp 3 Pt 1):S651; 4. Johnson JT, et al. Pharm Res. 2001;12 (Supp 9):S387; 5. Cymbalta SPC.
Hepatic Safety Profile of Duloxetine • Metabolized by CYP2D6 and 1A21 • Moderate inhibitor of 2D6 • No clinically significant inhibition of 1A2, 3A, 2C9, or 2C19 • No induction of CYP isoenzymes • In the overall duloxetine clinical trial database (N=3,372), just three duloxetine-treated patients met laboratory thresholds predictive of liver injury1 • No specific laboratory tests are recommended, although duloxetine should ordinarily not be prescribed to patients with substantial alcohol use nor patients with any hepatic insufficiency1 1. Cymbalta US Prescribing Information.
Duration* 4 days5 days6 days Duration* 23 days13 days15 days • *Median duration data: • Placebo • Duloxetine (60 mg) • Duloxetine (120 mg) Duration* 5 days4 days 6 days Most Common Adverse Events Associated with Duloxetine in DPNP Pooled data from 3 studies Cymbalta Adverse Events that Occurred 5% and Twice Placebo Placebo (n=339) Duloxetine 20 mg/day (n=115) Duloxetine 60 mg/day (n=334) Duloxetine 120 mg/day (n=341) % Incidence of Adverse Events Nausea Somnolence Dizziness Constipation Sweating Dry Mouth Appetite Poster: Robinson M, et al. Presented at: 8th International Conference on the Mechanisms and Treatment of Neuropathic Pain (ICMTNP); San Francisco, CA; Nov 5, 2005.
50 Nausea 40 30 20 10 0 1 2 3 4 5 6 7 8 9 10 11 12 50 Somnolence 40 30 20 10 0 1 2 3 4 5 6 7 8 9 10 11 12 50 Dizziness 40 30 20 10 0 1 2 3 4 5 6 7 8 9 10 11 12 Placebo (n=339) Cymbalta 60 mg/day (n=334) Cymbalta 120 mg/day (n=341) Clinical Profile of the 3 Most Common Adverse Events Pooled data from 3 studies Onset Median Duration Severity (60 mg/QD) 9% 2% 13% Duloxetine 60 mg/day=5 daysDuloxetine 120 mg/day=6 days Placebo=4 days 76% 2% 3% 12% Duloxetine 60 mg/day=13 daysDuloxetine 120 mg/day=15 days Placebo=23 days 85% % Patients Reporting AE (New Cases) 1% 3% 6% 90% Duloxetine 60 mg/day=4 daysDuloxetine 120 mg/day=6 days Placebo=5 days Weeks Mild Severe Moderate None Poster: Robinson M, et al. Presented at: 8th International Conference on the Mechanisms and Treatment of Neuropathic Pain (ICMTNP); San Francisco, CA; Nov 5, 2005.
Nausea on Duloxetine is Common, but is Short-Lived and Mostly Mild or Moderate Pooled data from 3 studies Severity of Treatment-emergent Nausea on Duloxetine 60 mg QD Severe 2% Moderate 9% Mild 13% None 76% • Of all the DPNP patients reporting nausea, 92% reported it as mild to moderate • Nausea occurred primarily during the first week of treatment and resolved rapidly with continued treatment (median duration 5 days) Poster: Robinson M, et al. Presented at: 8th International Conference on the Mechanisms and Treatment of Neuropathic Pain (ICMTNP); San Francisco, CA; Nov 5, 2005.
No Evidence of an Increased Risk of Suicidality with Duloxetine • The data from studies of adult patients with MDD demonstrate that duloxetine significantly reduces the risk of worsening suicidal ideation and significantly increases the chances for improvement in ideation for patients who had suicidal ideation at baseline. • The data from studies of adult patients with nonpsychiatric indications (including SUI, FM and DPNP) support the conclusion that duloxetine is not associated with the development of suicidal ideation in depressed or non-depressed adult patients receiving duloxetine for any of the indications. NOTE: The duloxetine FDA black box warning about suicidality in adults is derived from a meta-analysis of all drugs in this class. Although primarily based on studies of MDD, the warning applies to all indications. Data on file.
Depression as co-morbidity in patients with diabetes: • People with diabetes are twice as likely to be depressed as people without chronic disease. • Depression is a risk factor for onset of type 2 diabetes. • Improvement of depression ↔ improvement in glycemic control. • Psychological maladjustment or depression in diabetes can result from diabetes complications
Contents • Introduction • Mechanism of Action • Efficacy in DPNP • Pharmacokinetics, Safety and Tolerability • Conclusion
Summary • DPNP is a relatively widespread condition that significantly impacts patients’ functioning and quality of life • Duloxetine, a potent and balanced dual 5-HT and NE reuptake inhibitor, has been shown to significantly decrease pain in DPNP patients • Following 8 weeks of acute therapy, duloxetine 60 mg once daily maintained its efficacy in the management of diabetic peripheral neuropathic pain for 26 weeks. • Duloxetine is safe and well-tolerated