Download
1 / 27
700 likes | 2.32k Views
Bifurcation Stenting: A primer. Creighton Don, MD Assistant Professor of Cardiology University of Washington. Bifurcation lesions. Why How The data…. Bifurcation lesions:why. Large side branch supplying a reasonable territory Left main Cx -large OM LAD-large diag Ostial Cx /LAD

E N D
Bifurcation Stenting: A primer Creighton Don, MD Assistant Professor of Cardiology University of Washington
Bifurcation lesions • Why • How • The data…
Bifurcation lesions:why • Large side branch supplying a reasonable territory • Left main • Cx-large OM • LAD-large diag • OstialCx/LAD • RCA-PDA-PLV • Disease in the main branch and ostium/proximal side branch • Concern for losing the side branch • Rescuing dissected/occluded/jailed side branch
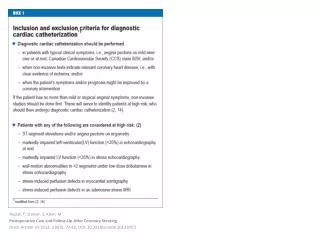
Bifurcation lesions: HOW Step 1: Classify lesion • Location of disease (Medina classification) • Extent of disease (focal?) • Size of prox/distal main branch and side branch • Angulation of side branch “True Bifurcation” lesion Levy MS, Moussa ID. “Bifurcation Lesions and Interventions,” in SCAI Interventional Cardiology Board Review. 2nd ed. 2013. Sgueglia GA. Chevalier B. JACC Cardio Interv. 2012.
Bifurcation lesions: HOW Step 2: Decide on approach • Not true bifurcation, side branch expendable or diffusely diseased, or not technically possible • Provisional • True bifurcation and suitable for stenting • V-stenting • Simultaneous Kissing Stents • T-stenting • Crush • Mini-crush • Reverse crush • Tap • Culotte
Provisional stenting • Side branch free of disease, too small, too diseased 1. Wire main branch +/- side branch for “protection” 2. Stent main branch 3. Assess flow in side branch—IF compromised: 4. Rewire side branch and PTCA, culotte, T-stent, reverse crush, TAP Louvard V. Catheterization and Cardiovascular Interventions71, (2)175-183, 2007.http://onlinelibrary.wiley.com/doi/10.1002/ccd.21314/full#fig1
Recrossing HR: 2.34, 95% confidence interval [CI]: 1.78 to 4.32, p < 0.001).
V-stenting • No disease proximal to the branch • Medina 0,1,1 • Angle < 90 degrees • No loss of side branch, no recrossing
Simultaneous kissing stentsDouble barrel • Larger proximal vessel, smaller distal/side branch • Simple to position/deploy, no loss of access, no recrossing • Neocarina • Challenging to recross, reintervene • Increased thrombosis/restenosis?
Crush, Mini-Crush • Treats side/main branch without losing access • Can treat size mismatched vessels • Good for shallow angle bifurcation • Complete coverage of carina • Lots of metal over side branch/carina • Difficult to recross • More restenosis 1. Position both stents 2. Inflate side branch stent 3. Inflate main branch stent (Crush) 4. Recross and kiss
Reverse Crush • Bail out for provisional stenting • May be difficult to recross side branch stent • Insures coverage of carina • Doesn’t commit to bifurcation stent from beginning 1. Stent main branch 2. Wire and stent side branch 3. Crush side branch stent with a balloon in the main branch 4. Recross and kiss 4 2 3 1
T-Stenting • Simple, can treat size mismatched vessels • Can lose one branch while treating the other • Need to recross stent • Good for angles closer to 90 degrees • Uncovered carina (<90 degrees) • If the side stent is deployed into the main branch, then this may be called a “mini-crush or a modified-T stent
Culotte • Complete coverage • Good for shallow angle, harder for steep angle • Loses access to alternate branch twice • Recross stents twice • Requires relatively equal sized vessels • Difficulty advancing 2nd stent 1. Stent one branch 2. Wire and stent other branch 3. Recross original branch and kiss
T-stenting with protrusion (TAP) Latib A, Columbo A. Controversies and Consensus in Imaging and Intervention. Vol 5, 2, 2007.
Bifurcation stenting: why? • Pro: • Protects side branch • Reduces ischemic burden • Easier at the time of the PCI • May not be able to salvage side branch after main branch is stented • Con: • More time, radiation, contrast • More restenosis • Jeopardizes the main branch • Side branch lesion often not significant • Side branch often stays open
BMS vsDES: One vs. two stents Latib A, Columbo A. Controversies and Consensus in Imaging and Intervention. Vol 5, 2, 2007.
DES: One vs. two stents NS Latib A, Columbo A. Controversies and Consensus in Imaging and Intervention. Vol 5, 2, 2007.
Nordic bifurcation studies • Nordic I: Provisional versus 2 stent • 70% with ‘true bifurcation’ lesions • Similar procedural success, longer fluoro/procedure time • Increased biomarker elevations MACE Stent thrombosis Steigen TK et al. Circulation. 2006;114:1955-1961
Meta-analysis Brar SS, EuroIntervention. 2009 Sep;5(4):475-84
FFR of jailed side branches Nordic-Baltic Bifurcation Study III • Provisional stentingFFR if TIMI 3 flow • Randomized to kissing or no kissing Post-PCI 8-mo % stenosis FFR KumsarsI, Narbute I, Thuesen L, et al. Side branch fractional flow reserve measurements after main vessel stenting: a Nordic-Baltic Bifurcation Study III substudy. EuroIntervention 2012;7:1155– 61.
To Kiss or not to kiss Sgueglia GA. Chevalier B. JACC Cardio Inter. 2012.
Balloon size for kissing Sgueglia GA. Chevalier B. JACC Cardio Inter. 2012.
AHA/ACC/SCAI Guidelines • CLASS I: Provisional side-branch stenting should be the initial approach in patients with bifurcation lesions when the side branch is not large and has only mild or moderate focal disease at the ostium. (Level of Evidence: A) • CLASS IIa: It is reasonable to use elective double stenting in patients with complex bifurcation morphology involving a large side branch where the risk of side-branch occlusion is high and the likelihood of successful side-branch reaccess is low. Levine GN et al. JACC. Volume 58, Issue 24, December 06, 2011
Dedicated bifurcation stents • Stentys • Nitinol and cell design allow for side branch expansion • Tryton • Open cells in main branch allowing a “culotte” • Sideguard • Nitinol stent, ostium flares allowing “T-stenting” • Antares II • Double lumen stent, maintain side branch access
Take home points • Keep it simple—use a provisional approach whenever possible • If you’re unsure, wire the side branch ahead of time • If the side branch needs to be ballooned, end with a kiss • BUT, TIMI 3 flow and <50% stenosis can be left alone • Consider FFR if you’re on the fence • Large side branches with disease >5 mm likely require 2-stent strategy • Difficult to access side branch may favor 2-stent strategy • True complicated bifurcations will be easier to treat with a two stent strategy if you plan ahead • E.g. recrossing into a diseased/jailed/occluded side branch can be challenging and upsizing your guide is painful • Pull your trapped wires before post dilating (keep track of your wires) Hildick-Smith D et al. EuroIntervention. 6 (1). 2010.